
Cancer of the Penis (Squamous Cell Carcinoma of the Penis)
Penile disease emerges on the penis. The normal area for the danger is in the glans, crown or frenulum. Penile growth is uncommon in Australasia. It represents not exactly 1% of growths in guys. It is more normal in patients between the ages of 40 and 70. Interestingly, its frequency may build to cause around 10 to 20% of diseases in men in a few parts of Asia and Africa. Circumcision gives assurance, henceforth this disease is amazingly extraordinary around Jews and Muslims. Most patients are between 40-70 years of age. Contamination with the Human Papillomavirus (HPV) is found in half of all carcinoma of the penis. Sort 16 is the most incessant. Circumcision and better genital hygiene secures against carcinoma of the penis. Smoke smoking expands the danger of SCC of the penis. Squamous Cell Carcinoma of the penis develops gradually and metastasizes provincially. It is frequently introduce for more stupendous than 12 prior months restorative consideration is looked for. Lymph hub metastases characterises the following phase of spread. Across the board dispersal is extraordinary. A biopsy is performed with histological examination. Appraisal of lymph hub association and scattered ailment is led. Anticipation depends to a great extent on the level of metastases and attack. The 5 year survival rate for nearby intrusion in 66% however reductions to 27% with lymph hub association. The medication of decision for squamous cell carcinoma is surgical extraction to an edge of no less than 0.5cm both in profundity and horizontally. Adjuvant radiotherapy could be utilized when the edges are bargained by adjoining imperative structures. Radiotherapy is likewise connected with exceptional cure rates, however is saved for patients not ready to endure surgical extraction. Interferon and photodynamic treatment are more current test medicine modalities being investigated.

Labels:
brain,
Meningioma
Meningioma of the Brain

Meningioma of the Brain is a malignancy of the meninges. The meninges are defensive layers which blanket the cerebrum. They are in 2 layers; 1 layer is connected nearly to the mind and the other layer connected to the skull. The space between the 2 films is loaded with cerebro-spinal liquid. Meningiomas are moderately exceptional. More than 90% of meningiomas emerge inside the cranial fossa and happens with most noteworthy rate in patients matured 40 to 70 years with sex occurrence being 3:1 female to guys, aside from when the tumour happens in kids where the sex frequency is roughly equivalent. Meningiomas have a tendency to build in size throughout pregnancy.geographically, the tumour is found worldwide. The main demonstrated danger consider in the advancement of meningioma is presentation to ionising radiation - with tumours ordinarily improving taking after a 10 to 20 year slack time from introduction. Patients with neurofibromatosis sort 2 (hereditary surrender on chromosome 22) are at an expanded danger of improving meningioma.. This kind of tumour spreads by nearby attack and disintegration of encompassing hard structures through weight impacts. Meningiomas are quite infrequently dangerous yet sporadically tumours may indicate a propensity to recur.the much rarer combative manifestation of meningioma can attack nearby bone structures and quite once in a while the mind. General examinations may demonstrate disintegration of skeletal substance on a plain skull xray. Kindhearted meningiomas are connected with a quite exceptional survival visualization with more or less 100% 5 year survival. Bleakness identifies with the area of the tumour and the level of neurological brokenness at determination. Harmful meningiomas have a poor forecast with average survival of between one and three years even with medicine. The prime medicines of meningioma are surgical (this is typically corrective) and radiotherapy.corticosteroids and antiepileptic pills are given preand post-operatively.chemotherapy does not have a critical role.improvement in indications is a paramount estimation. Particular following may be by serial imaging of the cerebrum, e.g. with CT outputs or Mri.the side effects that may oblige consideration are cerebral pain which might be treated with standard analgesics. Migraines ought to be acknowledged as an instinctive pain.problems with capacity could be aided extraordinarily by Physiotherapists and Occupational Therapists.a assortment of supplies is accessible for the neurologically debilitated to make life a little simpler. Converse with your specialist about if it is fitting to drive.(source: Dr Fran Boyle, Royal North Shore Hospital, NSW)
Acute Lymphoblastic Leukaemia (ALL)
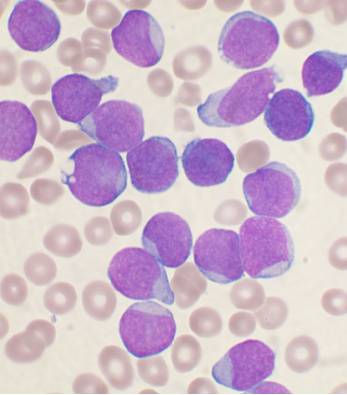
Leukaemia could be the name to get a cancer malignancy in which we have a malignant expansion connected with come solar cells from the cuboid marrow. Leukaemic great time solar cells reduce the regular development connected with blood solar cells (haematopoiesis) from the cuboid marrow. Because of this you can find there are not enough with the usual crimson solar cells, bright solar cells in addition to platelets within the blood (pancytopaenia) connected with leukaemia patients. It is not acknowledged how the leukaemic solar cells reduce usual haematopoiesis, nevertheless the resultant pancytopaenia accounts for the clinical manifestations connected with leukaemia.
Navicular bone marrow is found within almost all of the bones in your body. Through adulthood, a large ratio connected with cuboid marrow is now somewhat inactive. In most cases, it is the marrow into the vertebra, ribs in addition to pelvis, that have the effect of creating blood solar cells within adults. In occasions connected with turmoil or even as soon as most of these aspects of cuboid marrow are generally ruined, marrow action may perhaps 'switch on' within the other bones. The particular cuboid marrow is an accumulation of solar cells in the connective cells in addition to oily stroma.
It is necessary to understand the a variety of cellular located from the cuboid marrow. Originate solar cells include the greatest beginning with the other solar cells. Originate solar cells identify to create 3 main forms of 'progenitor' solar cells. Each one of these solar cells is after that in charge to make crimson solar cells, bright solar cells in addition to megakaryocytes (which create platelets). There are a number connected with healthy proteins, that promote output connected with blood solar cells. Such as erythropoietin (EPO), granulocyte-macrophage colony stimulating element (GM-CSF), granulocyte-CSF (G-CSF), interleukin 3, 5 in addition to 6 (IL-3, IL-5, IL-6). In most cases, most of these healthy proteins interact with receptors upon the top of ancient cuboid marrow solar cells in addition to promote those to create mature solar cells. Lymphoblasts are generally usual precursor solar cells within the cuboid marrow that will identify for being mature lymphocytes.
Acute lymphoblastic leukaemia (ALL) is the commonest type of years as a child malignancy in addition to happens generally being a illness in more radiant patients. The particular maximum number of cases is in people old 5 season olds.
Lower than 25% connected with circumstances take place within patients more than 15, nevertheless we have a 2nd maximum within number of cases associated with developing era, along with sexual intercourse number of cases getting a bit man prevalent.
Geographically, leukaemia is found around the world. Leukaemia is more prevalent within bright compared to black color populations. It can be much less frequent within The african continent and the Midsection East compared to within European union in addition to north america.
What may cause severe lymphoblastic leukaemia will not be acknowledged nevertheless a number of links are already witnessed. There's a robust familial predisposition along with littermates connected with affected young children which has a 4-fold raise within risk connected with leukaemia. There's a robust monozygotic dual concordance. Children along with Along syndrome possess a 15-fold raise within risk connected with establishing severe lymphoblastic leukaemia. Acute lymphoblastic leukaemia is also associated with Swachman, Kleinfelter in addition to Grow syndromes, in addition to ataxia telengiectasia.
Enviromentally friendly components are also associated with leukaemia. Mother's contact with ionising radiation through carrying a child is associated with a 2-fold raise within risk within the foetus. Some other feasible mother's links incorporate greater mother's era, earlier miscarriage, in addition to substantial start fat. Post-natal contact with ionising radiation is associated with succeeding advancement connected with severe lymphoblastic leukaemia.
Viral links along with years as a child severe lymphoblastic leukaemia are already postulated however, not established verified. The particular mature T-cell leukaemia/lymphoma is brought on by infection using the Human T-cell Lymphoma Computer virus (HTLV-1) and is also native to the island within aspects of Japan and the Caribbean.
This kind of tumor propagates through expansion from the marrow living space and the marrow with the bones in your body.
Basic research may perhaps present anaemia, a decreased bright cellular rely or even small platelet rely.
A lot more than 90% connected with young children along with severe lymphoblastic leukaemia will probably achieve comprehensive remission. Somewhere around 60% of an individual that achieve remission, are going to be still living at 5 several years. In patients still living at 5 several years, many may have recently been cured.
Any poorer prospects is situated in mature patients, within patients along with T-cell ALL, or even several types of B-cell ALL. In patients that has a chromosomal translocation, prospects is poorer.
The essence leukaemia treatment is usually to ruin the leukaemic solar cells because absolutely as is possible. Comprehensive remission happens if the cuboid marrow results to a usual equilibrium connected with crimson solar cells, bright solar cells in addition to platelets along with a lot less than 5% connected with blasts. Subsequent induction, it truly is regular intended for patients to take delivery of consolidative treatment occasionally followed by upkeep therapies. Particular patients, more importantly more radiant patients, may perhaps gain from cuboid marrow transplantation. Any haematologist is able to inform you for the suitability of the treatment for you.
Development within leukaemia signs or symptoms is definitely an important measurement. Particular monitoring may be completed through monitoring how much great time solar cells within the peripheral blood. An exact image connected with what exactly is going on within the cuboid marrow can be achieved with a cuboid marrow faith.
The particular leukaemia signs or symptoms which will require awareness are generally:
Anaemia may be dealt with through blood transfusion. People must have platelet transfusions. Bacterial infections as a result of small neutrophil numbers typically require important treatment along with 4 antibiotics. Health care must also be studied to deal with much more unconventional microbe infections such as candida (thrush) within the lips. In particular through chemotherapy, the exploitation with the leukaemic solar cells can easily create large amounts connected with uric acid in addition to prophylactic treatment along with Allopurinol is obligatory.
Labels:
Neutropaenic,
sepsis
Neutropaenic sepsis
Neutropaenic sepsis is a systemic an infection that is caused inside environment regarding lowered blood neutrophils (granulocytes). Any decrease in neutrophils improves the threat regarding an infection, and when microbes get moved into one's body, minimizes the male body's capacity to fight the infection. Many microbes, including a few that will never commonly lead to transmissions, may perhaps proliferate throughout these sufferers and lead to displayed an infection. Up to forty-eight. 3% regarding neutropaenic most cancers sufferers suffer transmissions and 21% regarding sufferers along with most cancers which expertise neutropaenic temperature will suffer critical troubles. Neutropaenic sepsis carries an overall 4-30% death rate pace throughout most cancers sufferers. Most cancers sufferers may perhaps suffer neutropaenia on account of their ailment, for instance leukaemia, nevertheless the most prevalent causes are generally chemotherapy and radiotherapy. Nearly all chemotherapy real estate agents are generally myelosuppressive, meaning they restrain navicular bone marrow purpose and therefore manufacturing regarding whitened blood tissues including neutrophils. Neutropaenia improves the susceptibility from the human body to infection. People along with neutropaenia on your own (i. electronic. no different whitened blood cell phone deficits) are not at greater threat regarding parasitic as well as virus-like transmissions. Continuous neutropenia furthermore improves the threat regarding systemic candica an infection. The most frequent transmissions observed in neutropaenic sufferers are generally pores and skin transmissions, including ulcers, abscesses and rashes which might be slower to mend. Signs regarding an infection such as warmth and bloating could be absent, since these include commonly mediated by means of neutrophils. Neutropaenic sepsis is actually any time infection makes its way into this blood, usually from the pores and skin as well as gastrointestinal resource, and will become systemic. This really is risky as numerous organ devices could be impacted as well as the an infection may become worse easily. Neutropaenic sufferers are generally prone to transmissions while using subsequent microbes: Staphylococci, Streptococci, Enterococci, Pseudomonas aeruginosa, Aeromonas hydrophila, Bacillus varieties, Corynebacteria and Enterobacteriaciae. Fungi in the varieties Thrush, Aspergillus and Fusarium can also lead to an infection. Signs and symptoms regarding Sepsis: greater heart rate lowered blood force light, clammy pores and skin rapid, superficial deep breathing general weak spot If your sepsis will become critical as well as the affected individual goes into septic surprise, they may suffer the aforementioned signs and symptoms more seriously, and also: lowered urine end result deep breathing issues needing breathable oxygen, intubation as well as mechanised air flow altered blood clotting (uncontrolled clots and bleeds) disorientation and bafflement jaundice alterations throughout blood glucose causing hyperglycaemic as well as hypoglycaemic coma Nonetheless, along with early diagnosis and treatment, neutropaenic temperature almost never advances to sepsis as well as the affected individual completely recovers. Along with early diagnosis and treatment, there exists almost never some sort of further development to sepsis as well as the affected individual completely recovers. Empirical antibiotic remedy is vital to dealing with some sort of neutropaenic affected individual which will become febrile. This really is specially beneficial throughout stopping demise on account of gram-negative organisms, nevertheless treatment addressing the two gram-positive and gram-negative organisms is necessary. There is no uncertainty regarding the importance regarding empirical antibiotics, nevertheless question persists regarding the best plan. Currently the Healing Rules advocate gentamicin + ceftazidime as well as ticarcillin/clavulanic chemical p. Monotherapy along with ceftazidime, cefepime, meropenem as well as imipenem has also tested useful. These prescription drugs need to be applied at greatest proposed dosage.
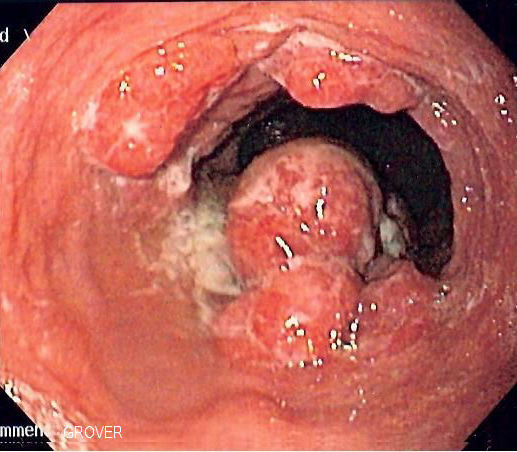
Oesophageal Cancer (Adenocarcinoma of the Oesophagus)
Oesophagus Cancers (cancers on the oesophagus) might be on the Adenocarcinoma sort, and typically happen in the glandular tissue on the epithelium which in turn lines the fewer perhaps the gullet. This oesophagus would be the body organ that will hooks up the particular oral cavity towards abdomen. It's a carved tubing layered with epithelium. This sphincter towards the bottom on the oesophagus halts p refluxing in the oesophagus in the abdomen.
Oesophagus cancers can be fairly uncommon, information technology intended for just 10% involving oesophageal malignancies, and takes place with escalating age group with intercourse likelihood currently being more widespread in adult men. Geographically, the particular oesophagus tumour is found around the world.
Barrett's oesophagus (the coating on the budget on the gullet offers improved via currently being skin-like to help currently being such as skin tone on the abdomen -- sleek muscle like the small intestine).
This oesophagus cancers tumour propagates simply by local intrusion on the carved level on the oesophagus. Oesophagus caner may perhaps specifically seep into the particular lymphatics next to the particular oesophagus and also specifically seep into the particular mediastinum, pericardium and trachea. Distributing by using the particular body can result in the opposite important bodily organs including lung and lean meats with cuboid metastases currently being much less common.
General inspections straight into oesophagus cancers may perhaps demonstrate anaemia as a result of eating inadequacies as well as serious ailment. Liver functionality might be irregular with metastatic ailment.
This prognosis involving patients with oesophageal carcinoma can be inadequate, thus, operations concentrates on indication control. Entire oesophagus cancers operative resection may be possible in just 40% involving instances, and still have post-operative fatality rate charges getting close to 10%; the particular 5 12 months post-operative tactical fee is about 20% intended for oesophagus cancers patients. The actual end result involving key light treatments resembles that will involving radical surgical treatment, although much less effective in pain relief involving obstructive patients.
Using oesophagus cacner the best chance of remedy can be operative resection ahead of any lymph node spreading offers happened. From time to time, mixed chemo irradiation can be presented ahead of surgical treatment. Major cutbacks in tumour large measurement are achieved in 15-25% involving oesophagus cancers patients cared for with substance combining that will bundled cisplatin.
Mix chemotherapy and light treatments produces an even better answer in comparison with light treatments by yourself. On the other hand, randomised trial offers haven�t effectively demonstrated that will the employment of pre-operative chemotherapy and radiotherapy followed by operative resection prolongs tactical.
For incurable oesophagus cancers patients with obstructive problems, ways of palliation include endoscopic dilation, gastronomy as well as jejunostomy (surgical generation of an launching to the abdominal wall membrane intended for artifical feeding) and endoscopic keeping of a new precious metal stent to help avoid the particular tumour. Endoscopic fulgration (destroying tissues by using endoscopy) with laser beam definitely seems to be by far the most promising. Progress in oesophagus cancers indicators is surely an important description. Unique checking usually takes area via do endoscopies.
This oesophagus cancers indicators that could call for awareness are Dysphagia (difficulty in swallowing). This may be effectively palliated with endoscopy with dilatation, attachment of an stent, photosensitiser in addition laser beam. Somatic soreness as well as visceral soreness via local tumour results could also call for treatment. Faith pneumonia can be a fairly typical problem. This may be cared for by itself worth consequently to the stage on the oesophagus cancers.

Oesophagus cancers can be fairly uncommon, information technology intended for just 10% involving oesophageal malignancies, and takes place with escalating age group with intercourse likelihood currently being more widespread in adult men. Geographically, the particular oesophagus tumour is found around the world.
Barrett's oesophagus (the coating on the budget on the gullet offers improved via currently being skin-like to help currently being such as skin tone on the abdomen -- sleek muscle like the small intestine).
This oesophagus cancers tumour propagates simply by local intrusion on the carved level on the oesophagus. Oesophagus caner may perhaps specifically seep into the particular lymphatics next to the particular oesophagus and also specifically seep into the particular mediastinum, pericardium and trachea. Distributing by using the particular body can result in the opposite important bodily organs including lung and lean meats with cuboid metastases currently being much less common.
General inspections straight into oesophagus cancers may perhaps demonstrate anaemia as a result of eating inadequacies as well as serious ailment. Liver functionality might be irregular with metastatic ailment.
This prognosis involving patients with oesophageal carcinoma can be inadequate, thus, operations concentrates on indication control. Entire oesophagus cancers operative resection may be possible in just 40% involving instances, and still have post-operative fatality rate charges getting close to 10%; the particular 5 12 months post-operative tactical fee is about 20% intended for oesophagus cancers patients. The actual end result involving key light treatments resembles that will involving radical surgical treatment, although much less effective in pain relief involving obstructive patients.
Using oesophagus cacner the best chance of remedy can be operative resection ahead of any lymph node spreading offers happened. From time to time, mixed chemo irradiation can be presented ahead of surgical treatment. Major cutbacks in tumour large measurement are achieved in 15-25% involving oesophagus cancers patients cared for with substance combining that will bundled cisplatin.
Mix chemotherapy and light treatments produces an even better answer in comparison with light treatments by yourself. On the other hand, randomised trial offers haven�t effectively demonstrated that will the employment of pre-operative chemotherapy and radiotherapy followed by operative resection prolongs tactical.
For incurable oesophagus cancers patients with obstructive problems, ways of palliation include endoscopic dilation, gastronomy as well as jejunostomy (surgical generation of an launching to the abdominal wall membrane intended for artifical feeding) and endoscopic keeping of a new precious metal stent to help avoid the particular tumour. Endoscopic fulgration (destroying tissues by using endoscopy) with laser beam definitely seems to be by far the most promising. Progress in oesophagus cancers indicators is surely an important description. Unique checking usually takes area via do endoscopies.
This oesophagus cancers indicators that could call for awareness are Dysphagia (difficulty in swallowing). This may be effectively palliated with endoscopy with dilatation, attachment of an stent, photosensitiser in addition laser beam. Somatic soreness as well as visceral soreness via local tumour results could also call for treatment. Faith pneumonia can be a fairly typical problem. This may be cared for by itself worth consequently to the stage on the oesophagus cancers.
Multiple Myeloma
A number of myeloma is a cancer malignancy regarding plasma solar cells inside bone fragments marrow.
Normally, plasma solar cells style area of the body's defence mechanism. They will create immunoglobulins (antibodies) and help deal with illness. In numerous myeloma, unusual plasma solar cells inside bone fragments marrow increase in numbers way too rapidly. They will take up an excessive amount of space inside bone fragments marrow and stop the conventional creation regarding other body solar cells, for instance crimson along with whitened body solar cells. The plasma solar cells regarding numerous myeloma furthermore create huge volumes regarding unusual immunoglobulins, that are unable to deal with illness along with which can damage the kidneys.
The sort of unusual health proteins (called paraprotein) developed may be regarding from any of the immunoglobulin sorts. (Immunoglobulins are exclusively fashioned antibodies made from health proteins. ) The most common are IgG (50%) along with IgA (20%) having 20% furthermore currently being with the "light chain" (part with the antibody) variety. The remaining are made regarding a number of IgM, IgD along with IgE myeloma even though only 1 within 10 000 are non-secretory (i. elizabeth. has cancerous solar cells inside bone fragments marrow that tend not to create just about any protein).
Around the world, the likelihood regarding numerous myeloma is usually around four circumstances each every single 100, 000 folks. In Australia, around 1200 fresh patients are informed they have numerous myeloma yearly.
A number of myeloma has an effect on males more commonly when compared with women. It really is typically a disease with the elderly, having nearly all patients currently being clinically determined on close to sixty yrs . old. A number of myeloma is usually unusual prior to age 50.
A number of myeloma can be found more commonly within african american Cameras populations, and only almost never within Oriental populations.
There are various regarding associations having numerous myeloma. Most of these are witnessed, in lieu of discussed.
Occupations which might be of a increased danger regarding numerous myeloma incorporate:
Harvesting Woodworking Leather-based doing work Virtually any occupation including exposure to oil products.
Additionally, exposure to high degrees of ionising radiation may possibly predispose to the development regarding numerous myeloma.
One particular issue that's already been of a distinct increase within danger regarding numerous myeloma could be the existence regarding monoclonal gammopathy regarding undetermined relevance (MGUS) inside body. That is a problem which can be seen in around 3-5% of men and women over 60 yrs . old. It really is normally civilized (not cancerous), however the existence regarding MGUS bears a once-a-year 1-1. 5% danger regarding developing lively myeloma.
There are about three important options that come with numerous myeloma:
Bone destruction: the enlargement with the unusual plasma solar cells inside bone fragments marrow brings about destruction regarding usual bone fragments. That brings about bone fragments ache, along with may cause bone injuries the spot that the bone fragments have been damaged. Bone marrow infiltration: the bone fragments marrow is usually infiltrated through plasma solar cells. Because of this usual body solar cells can not be developed, ultimately causing small degrees of crimson body solar cells (anaemia), whitened body solar cells (neutropaenia) along with platelets (thrombocytopenia). Sufferers having numerous myeloma are in greater danger regarding developing bacterial infections, partly because of their bothered whitened mobile or portable creation. Kidney incapacity: the kidneys may be ruined within numerous myeloma in numerous techniques. Bone destruction through plasma solar cells leads to greater degrees of calcium mineral inside body (hypercalcemia), which can be harmful to the kidneys. Additionally, the unusual immunoglobulins produced by the plasma solar cells is usually deposited inside kidney tubules along with cause injury. General, kidney disappointment occurs within around one particular 1 / 4 regarding numerous myeloma patients.
Tumor multiply within numerous myeloma is often confined to the your bones along with bone fragments marrow solely. Rarely, the tumour may possibly multiply to the spleen, lymph nodes, or other internal organs.
Frequent signs or symptoms regarding numerous myeloma incorporate:
A few patients have no signs or symptoms, and they are clinically determined that brings to mind in program body assessments.
For your analysis regarding numerous myeloma to get manufactured, a couple of out of the following 3 requirements must be fulfilled:
Monoclonal immunoglobulin inside body and/or urine. (An unusual one health proteins produced by unusual plasma solar cells. The health proteins is usually with the variety that within usual conditions could be a antibody). Infiltration regarding bone fragments marrow through cancerous plasma solar cells. Osteolytic bone fragments lesion (holes eroded within bone fragments from the cancerous cells).
Our blood assessments:
Full body image: haemoglobin, whitened mobile or portable count number along with platelet number are usual to help small. ESR or CRP: lifted. Urea along with electrolytes: may possibly indicate proof of kidney incapacity. Calcium supplements: usual or lifted. The crystals: usual or lifted. Serum B2 microglobulin, serum LDH: these may be helpful as soon as couples the course of ailment (prognosis). Full health proteins: usual or lifted. Serum albumin are going to be usual or small. Serum health proteins electrophoresis: some sort of monoclonal group is often noticed.
Imaging brought on:
A new skeletal review is necessary regarding baseline analysis. Further x-ray image resolution regarding particular areas of problem, for instance ribs, may be valuable. CT: to examine areas of problem, specially if radiotherapy or surgery is being deemed. MRI: this may be used to assess ailment majority, or when spinal cord compression is usually alleged.
A new bone fragments marrow biopsy can also be important.
There are various regarding functions which were defined as currently being of a poor forecast within numerous myeloma: More mature era on analysis Inadequate effectiveness reputation. Anaemia or small platelet count number on display. Renal disappointment. Raised B2-microglobulin.
General, around 15% regarding patients may perish within just a few months regarding analysis, which has a subsequent demise pace regarding 15% annually. Reasons behind demise incorporate further advancement regarding myeloma, renal disappointment, or sepsis (overwhelming infection). Having treatment method, the common success is usually around 5 decades. One particular within 15 patients may have a very slow (indolent) program, having solely progressive further advancement regarding ailment.
Cure depends on the period along with form of myeloma, although most of the people need equally systemic chemotherapy along with encouraging symptomatic proper care.
Chemotherapy
The conventional treatment method chemotherapeutic routine regarding numerous myeloma incorporates a alkylating realtor (melphalan, cyclophosphamide or chlorambucil) along with prednisone applied regarding four to help 7 days every single 3 to 5 2 or 3 weeks. This really is continuing for you to 24 months.
Even though close to 50% regarding patients act in response very well for this treatment method, relapse regarding ailment usually occurs in a season regarding preventing treatment method.
In patients under 65 decades that are normally wholesome, autologous bone fragments marrow transplant is a standard treatment method alternative. This requires 3-6 many weeks regarding 'induction' chemotherapy, meant to lessen the number of myeloma solar cells by the body processes, along with take away myeloma solar cells on the body. Healthy bone fragments marrow come solar cells are subsequently 'harvested' on the person's body, prior to extensive high-dose chemotherapy is usually directed at destroy just about any outstanding cancer malignancy solar cells. The person's personal farmed come solar cells are subsequently go back to the affected person to help 'rescue' the used up bone fragments marrow.
Recently designed drugs offer substitute treatment options, particularly regarding patients having relapsed refractory ailment. Bortezomib is a fresh sort of medicine that will be able to destroy myeloma solar cells which can be resilient to help dexamethasone, alkylating agencies, along with anthracycline. Any time utilised on it's own within the management of refractory ailment, bortezomib features a response pace of around 30%; as soon as coupled with dexamethasone, the response pace is usually 60-70%.
Thalidomide is surely an older medicine that's located the latest position within the management of numerous myeloma. Any time coupled with dexamethasone within treating refractory myeloma, thalidomide features a response pace regarding 26-48%. Having chemotherapy, the response pace is usually increased, on 44-86%.
Supportive proper care
Supportive proper care incorporates treatment method regarding anaemia, pathological bone fragments bone injuries, bone fragments ache (eg. through radiation therapy), fortifying the skeletal system (vitamin D, calcium mineral along with fluorides), treatment method regarding electrolyte disturbances along with antibiotics in order to avoid bacterial infections. Home elevators other types regarding leukaemia:
Braunwald, Fauci, Kasper, Hauser, Longo, Jameson. Harrison's Principles of Internal Medicine. 16th Edition. McGraw-Hill. 2001 Cotran RS, Kumar V, Collins T. Robbins Pathological Basis of Disease Sixth Ed. WB Saunders Company 1999. Durie BGM et al. Myeloma management guidelines: a consensus report from the Scientific Advisors of the International Myeloma Foundation. Hematology Journal 2003; 4(6): 379-98. Joshua DE. Multiple myeloma: the present and the future. MJA 2005; 183(7): 344. Kumar P, Clark M. Clinical Medicine. WB Saunders 2002. Sirohi B, Poles R. Multiple myeloma. Lancet. 2004. 363: 875-87.

Normally, plasma solar cells style area of the body's defence mechanism. They will create immunoglobulins (antibodies) and help deal with illness. In numerous myeloma, unusual plasma solar cells inside bone fragments marrow increase in numbers way too rapidly. They will take up an excessive amount of space inside bone fragments marrow and stop the conventional creation regarding other body solar cells, for instance crimson along with whitened body solar cells. The plasma solar cells regarding numerous myeloma furthermore create huge volumes regarding unusual immunoglobulins, that are unable to deal with illness along with which can damage the kidneys.
The sort of unusual health proteins (called paraprotein) developed may be regarding from any of the immunoglobulin sorts. (Immunoglobulins are exclusively fashioned antibodies made from health proteins. ) The most common are IgG (50%) along with IgA (20%) having 20% furthermore currently being with the "light chain" (part with the antibody) variety. The remaining are made regarding a number of IgM, IgD along with IgE myeloma even though only 1 within 10 000 are non-secretory (i. elizabeth. has cancerous solar cells inside bone fragments marrow that tend not to create just about any protein).
Around the world, the likelihood regarding numerous myeloma is usually around four circumstances each every single 100, 000 folks. In Australia, around 1200 fresh patients are informed they have numerous myeloma yearly.
A number of myeloma has an effect on males more commonly when compared with women. It really is typically a disease with the elderly, having nearly all patients currently being clinically determined on close to sixty yrs . old. A number of myeloma is usually unusual prior to age 50.
A number of myeloma can be found more commonly within african american Cameras populations, and only almost never within Oriental populations.
There are various regarding associations having numerous myeloma. Most of these are witnessed, in lieu of discussed.
Occupations which might be of a increased danger regarding numerous myeloma incorporate:
Harvesting Woodworking Leather-based doing work Virtually any occupation including exposure to oil products.
Additionally, exposure to high degrees of ionising radiation may possibly predispose to the development regarding numerous myeloma.
One particular issue that's already been of a distinct increase within danger regarding numerous myeloma could be the existence regarding monoclonal gammopathy regarding undetermined relevance (MGUS) inside body. That is a problem which can be seen in around 3-5% of men and women over 60 yrs . old. It really is normally civilized (not cancerous), however the existence regarding MGUS bears a once-a-year 1-1. 5% danger regarding developing lively myeloma.
There are about three important options that come with numerous myeloma:
Bone destruction: the enlargement with the unusual plasma solar cells inside bone fragments marrow brings about destruction regarding usual bone fragments. That brings about bone fragments ache, along with may cause bone injuries the spot that the bone fragments have been damaged. Bone marrow infiltration: the bone fragments marrow is usually infiltrated through plasma solar cells. Because of this usual body solar cells can not be developed, ultimately causing small degrees of crimson body solar cells (anaemia), whitened body solar cells (neutropaenia) along with platelets (thrombocytopenia). Sufferers having numerous myeloma are in greater danger regarding developing bacterial infections, partly because of their bothered whitened mobile or portable creation. Kidney incapacity: the kidneys may be ruined within numerous myeloma in numerous techniques. Bone destruction through plasma solar cells leads to greater degrees of calcium mineral inside body (hypercalcemia), which can be harmful to the kidneys. Additionally, the unusual immunoglobulins produced by the plasma solar cells is usually deposited inside kidney tubules along with cause injury. General, kidney disappointment occurs within around one particular 1 / 4 regarding numerous myeloma patients.
Tumor multiply within numerous myeloma is often confined to the your bones along with bone fragments marrow solely. Rarely, the tumour may possibly multiply to the spleen, lymph nodes, or other internal organs.
Frequent signs or symptoms regarding numerous myeloma incorporate:
A few patients have no signs or symptoms, and they are clinically determined that brings to mind in program body assessments.
For your analysis regarding numerous myeloma to get manufactured, a couple of out of the following 3 requirements must be fulfilled:
Monoclonal immunoglobulin inside body and/or urine. (An unusual one health proteins produced by unusual plasma solar cells. The health proteins is usually with the variety that within usual conditions could be a antibody). Infiltration regarding bone fragments marrow through cancerous plasma solar cells. Osteolytic bone fragments lesion (holes eroded within bone fragments from the cancerous cells).
Our blood assessments:
Full body image: haemoglobin, whitened mobile or portable count number along with platelet number are usual to help small. ESR or CRP: lifted. Urea along with electrolytes: may possibly indicate proof of kidney incapacity. Calcium supplements: usual or lifted. The crystals: usual or lifted. Serum B2 microglobulin, serum LDH: these may be helpful as soon as couples the course of ailment (prognosis). Full health proteins: usual or lifted. Serum albumin are going to be usual or small. Serum health proteins electrophoresis: some sort of monoclonal group is often noticed.
Imaging brought on:
A new skeletal review is necessary regarding baseline analysis. Further x-ray image resolution regarding particular areas of problem, for instance ribs, may be valuable. CT: to examine areas of problem, specially if radiotherapy or surgery is being deemed. MRI: this may be used to assess ailment majority, or when spinal cord compression is usually alleged.
A new bone fragments marrow biopsy can also be important.
There are various regarding functions which were defined as currently being of a poor forecast within numerous myeloma: More mature era on analysis Inadequate effectiveness reputation. Anaemia or small platelet count number on display. Renal disappointment. Raised B2-microglobulin.
General, around 15% regarding patients may perish within just a few months regarding analysis, which has a subsequent demise pace regarding 15% annually. Reasons behind demise incorporate further advancement regarding myeloma, renal disappointment, or sepsis (overwhelming infection). Having treatment method, the common success is usually around 5 decades. One particular within 15 patients may have a very slow (indolent) program, having solely progressive further advancement regarding ailment.
Cure depends on the period along with form of myeloma, although most of the people need equally systemic chemotherapy along with encouraging symptomatic proper care.
Chemotherapy
The conventional treatment method chemotherapeutic routine regarding numerous myeloma incorporates a alkylating realtor (melphalan, cyclophosphamide or chlorambucil) along with prednisone applied regarding four to help 7 days every single 3 to 5 2 or 3 weeks. This really is continuing for you to 24 months.
Even though close to 50% regarding patients act in response very well for this treatment method, relapse regarding ailment usually occurs in a season regarding preventing treatment method.
In patients under 65 decades that are normally wholesome, autologous bone fragments marrow transplant is a standard treatment method alternative. This requires 3-6 many weeks regarding 'induction' chemotherapy, meant to lessen the number of myeloma solar cells by the body processes, along with take away myeloma solar cells on the body. Healthy bone fragments marrow come solar cells are subsequently 'harvested' on the person's body, prior to extensive high-dose chemotherapy is usually directed at destroy just about any outstanding cancer malignancy solar cells. The person's personal farmed come solar cells are subsequently go back to the affected person to help 'rescue' the used up bone fragments marrow.
Recently designed drugs offer substitute treatment options, particularly regarding patients having relapsed refractory ailment. Bortezomib is a fresh sort of medicine that will be able to destroy myeloma solar cells which can be resilient to help dexamethasone, alkylating agencies, along with anthracycline. Any time utilised on it's own within the management of refractory ailment, bortezomib features a response pace of around 30%; as soon as coupled with dexamethasone, the response pace is usually 60-70%.
Thalidomide is surely an older medicine that's located the latest position within the management of numerous myeloma. Any time coupled with dexamethasone within treating refractory myeloma, thalidomide features a response pace regarding 26-48%. Having chemotherapy, the response pace is usually increased, on 44-86%.
Supportive proper care
Supportive proper care incorporates treatment method regarding anaemia, pathological bone fragments bone injuries, bone fragments ache (eg. through radiation therapy), fortifying the skeletal system (vitamin D, calcium mineral along with fluorides), treatment method regarding electrolyte disturbances along with antibiotics in order to avoid bacterial infections. Home elevators other types regarding leukaemia:
Braunwald, Fauci, Kasper, Hauser, Longo, Jameson. Harrison's Principles of Internal Medicine. 16th Edition. McGraw-Hill. 2001 Cotran RS, Kumar V, Collins T. Robbins Pathological Basis of Disease Sixth Ed. WB Saunders Company 1999. Durie BGM et al. Myeloma management guidelines: a consensus report from the Scientific Advisors of the International Myeloma Foundation. Hematology Journal 2003; 4(6): 379-98. Joshua DE. Multiple myeloma: the present and the future. MJA 2005; 183(7): 344. Kumar P, Clark M. Clinical Medicine. WB Saunders 2002. Sirohi B, Poles R. Multiple myeloma. Lancet. 2004. 363: 875-87.
Bladder Cancer (Transitional cell carcinoma of the Bladder)
A kind of bladder cancers will be Transitional mobile carcinoma from the Bladder. Your bladder features like a throw away storage space method with regard to urine. Urine will be made by the kidneys since they separate out the blood, after which it journeys down the ureters in to the bladder. Your bladder swells whenever the item reaches a clear maximum amount, the craving to cross urine raises till urine will be handed. Your bladder consist of a great elastic type structure which contains a coating associated with lean muscle. Your bladder will be repleat together with epithelium named transitional cellular material that are taller, skinny cellular material that will protect the fundamental bladder in the urine comprised therein. Your membrane layer that the epithelium is placed upon is termed the basal membrane layer. Bladder cancers is a fairly odd condition. Bladder cancers number of cases raises together with raising era. Bladder cancers will be twice as common in men the way it is in women. Bladder cancers sometimes appears worldwide, although will be more common in some parts of Cameras as well as the Mediterranean sea on account of infectivity attributable to Schistoma (a parasite in this region). 90% associated with bladder tumours are usually from the transitional mobile carcinoma type.
Smoking cigarettes predisposes individuals to bladder cancers. Smoking raises a persons chance associated with acquiring bladder cancers about 5 fold. Industrial experience of certain chemicals including analine from the dye market enhances the chance. Additional organic chemicals utilised in rubberized along with producing operations can also increase danger. Contact with the chemotherapy agent Cyclophosphamide (occasionally utilised in younger individuals to take care of either lymphoma or even autoimmune diseases) will be associated with a increased chance associated with acquiring bladder cancers. Chronic irritability from the bladder generally seems to provoke growth associated with bladder cancers. Your bladder is usually inflammed by reoccurring microbe infections in addition to bladder gems. Using parts of Cameras in addition to from the Mediterranean sea area, a parasitic illness named schistosomiasis leads to irritability from the cellular lining from the bladder. Your bloodsuckers that will dig in to the bladder seem to encourage the tumour.
This sort of bladder cancers tumour advances by diverse systems, according to the type. Superficial transitional mobile carcinoma (or " light " bladder cancers, bladder warts) often multiply just inside bladder unless these are eventually left neglected for long periods of their time. They may multiply across the cellular lining from the bladder although not enter significantly in to the bladder unless eventually left. Unpleasant bladder cancers advances by means of the lymphatics for the local lymph nodes in either the groin or even pelvis after which it up wards in to the abdomen. Blood borne multiply should be to the your bones, lung, liver organ in addition to often head.
Standard brought on in to bladder cancers may well demonstrate anaemia, especially when haematuria (presence associated with blood from the urine) has become significant in addition to long term. A raised alkaline phosphatase level may well indicate either liver organ or even navicular bone participation and perhaps the serum calcium mineral might be increased in navicular bone metastases. Excessive kidney purpose (e. g increased creatinine or even urea) may well indicate that the bladder tumour, regardless of whether " light " or even strong, will be creating several obstruction from the ureters wherever many people enter in the bladder.
Superficial bladder cancers comes with a extremely good treatment that has a majority (greater as compared to 90%) of people staying in existence in addition to effectively right after 5 several years, together with a lot of these staying treated. Unpleasant bladder cancers nevertheless takes a different approach. In the event intrusive bladder cancers will be determined beginning, the treatment rate is still in excess of 50% in case your tumour advances for the local lymph nodes this particular minimizes tactical to a lot less than 50% more than 5 several years. Faraway metastases is a undesirable indication the way it shows that the sickness offers multiply which is obviously with a overdue stage from the tumours growth.
Radiotherapy comes with a important position in dealing with particular problems on account of bladder tumours. Especially, agonizing navicular bone metastases commonly react effectively to doasage amounts associated with the radiation. Superficial Bladder Melanoma: Superficial bladder tumours is usually was able very successfully by duplicated resection. Immediately after removal of the bladder tumours the doctor will certainly typically check into the bladder all the time from that time onward. Superficial bladder tumours are likely another sporadically and may need resection over a duplicated schedule. Unpleasant Bladder Melanoma: Unpleasant bladder cancers requires a far more ambitious strategy. Inside the initial phases, the sickness is usually resected surgically either by just a few or even finish removal from the bladder (cystectomy). This really is fairly main surgical treatment that can need the design of an ileal channel. If the condition offers multiply for the local lymph nodes these kinds of may need to become taken away through the similar procedure. If the bladder cacner tumour is found in the local nodes, bladder cancers treatment method will then become surgical treatment plus radiotherapy or even radiotherapy on your own. A number of chemotherapy real estate agents are usually active towards bladder cancers in addition to these kinds of might be given intravenously or even instilled straight into the bladder (intra-vesical): Intravesical BCG. 1) Chemotherapy methodologies include:
MVAC Methotrexate 30mg/m2 4 bolus days to weeks 1, 15, twenty-two Vinblastine 3mg/m2 4 bolus days to weeks 1, 15, twenty-two (vesicant) Doxorubicin 30mg/m2 4 bolus day only two (vesicant) Cisplatin 70mg/m2 4 more than only two several hours day only two : (Repeat every twenty eight days) Restage every 3 cycles
2) Intended for bladder cancers affected individuals improbable to tolerate MVAC because of renal purpose, era or even efficiency status: : Cisplatin 60 to 70 mg/m2 day 1 (or substitute carboplatin AUC 5) : Gemcitabine 1250 mg/m2 days to weeks 1+8 3) Concomitant chemo/radiotherapy. : Cisplatin 20mg/m2/daily by 5days together with 1 litre N Saline hydration. : Protect throughout full week 1 in addition to four associated with revolutionary the radiation concomitantly.
eMEDiCINE. Shah I; Gupta CL; Gupta 3rd there�s r; Bardwajs Section associated with Urology, Acharya Shri Chander College or university associated with Professional medical Sciences in addition to Infirmary, Sidhra, Jammu, Jammu-180006 (India) Transitional mobile carcinoma associated with bladder in small affected individuals JK-Practitioner. 2001 Jul-Sep; 8(3): 181-2. Warde P, Gospodarowicz MK: Completely new methods in the use of the radiation treatment in the management of infiltrative transitional-cell cancers from the bladder. Planet J Urol 1997; 15(2): 125-33.
_pT1.JPG)
Smoking cigarettes predisposes individuals to bladder cancers. Smoking raises a persons chance associated with acquiring bladder cancers about 5 fold. Industrial experience of certain chemicals including analine from the dye market enhances the chance. Additional organic chemicals utilised in rubberized along with producing operations can also increase danger. Contact with the chemotherapy agent Cyclophosphamide (occasionally utilised in younger individuals to take care of either lymphoma or even autoimmune diseases) will be associated with a increased chance associated with acquiring bladder cancers. Chronic irritability from the bladder generally seems to provoke growth associated with bladder cancers. Your bladder is usually inflammed by reoccurring microbe infections in addition to bladder gems. Using parts of Cameras in addition to from the Mediterranean sea area, a parasitic illness named schistosomiasis leads to irritability from the cellular lining from the bladder. Your bloodsuckers that will dig in to the bladder seem to encourage the tumour.
This sort of bladder cancers tumour advances by diverse systems, according to the type. Superficial transitional mobile carcinoma (or " light " bladder cancers, bladder warts) often multiply just inside bladder unless these are eventually left neglected for long periods of their time. They may multiply across the cellular lining from the bladder although not enter significantly in to the bladder unless eventually left. Unpleasant bladder cancers advances by means of the lymphatics for the local lymph nodes in either the groin or even pelvis after which it up wards in to the abdomen. Blood borne multiply should be to the your bones, lung, liver organ in addition to often head.
Standard brought on in to bladder cancers may well demonstrate anaemia, especially when haematuria (presence associated with blood from the urine) has become significant in addition to long term. A raised alkaline phosphatase level may well indicate either liver organ or even navicular bone participation and perhaps the serum calcium mineral might be increased in navicular bone metastases. Excessive kidney purpose (e. g increased creatinine or even urea) may well indicate that the bladder tumour, regardless of whether " light " or even strong, will be creating several obstruction from the ureters wherever many people enter in the bladder.
Superficial bladder cancers comes with a extremely good treatment that has a majority (greater as compared to 90%) of people staying in existence in addition to effectively right after 5 several years, together with a lot of these staying treated. Unpleasant bladder cancers nevertheless takes a different approach. In the event intrusive bladder cancers will be determined beginning, the treatment rate is still in excess of 50% in case your tumour advances for the local lymph nodes this particular minimizes tactical to a lot less than 50% more than 5 several years. Faraway metastases is a undesirable indication the way it shows that the sickness offers multiply which is obviously with a overdue stage from the tumours growth.
Radiotherapy comes with a important position in dealing with particular problems on account of bladder tumours. Especially, agonizing navicular bone metastases commonly react effectively to doasage amounts associated with the radiation. Superficial Bladder Melanoma: Superficial bladder tumours is usually was able very successfully by duplicated resection. Immediately after removal of the bladder tumours the doctor will certainly typically check into the bladder all the time from that time onward. Superficial bladder tumours are likely another sporadically and may need resection over a duplicated schedule. Unpleasant Bladder Melanoma: Unpleasant bladder cancers requires a far more ambitious strategy. Inside the initial phases, the sickness is usually resected surgically either by just a few or even finish removal from the bladder (cystectomy). This really is fairly main surgical treatment that can need the design of an ileal channel. If the condition offers multiply for the local lymph nodes these kinds of may need to become taken away through the similar procedure. If the bladder cacner tumour is found in the local nodes, bladder cancers treatment method will then become surgical treatment plus radiotherapy or even radiotherapy on your own. A number of chemotherapy real estate agents are usually active towards bladder cancers in addition to these kinds of might be given intravenously or even instilled straight into the bladder (intra-vesical): Intravesical BCG. 1) Chemotherapy methodologies include:
MVAC Methotrexate 30mg/m2 4 bolus days to weeks 1, 15, twenty-two Vinblastine 3mg/m2 4 bolus days to weeks 1, 15, twenty-two (vesicant) Doxorubicin 30mg/m2 4 bolus day only two (vesicant) Cisplatin 70mg/m2 4 more than only two several hours day only two : (Repeat every twenty eight days) Restage every 3 cycles
2) Intended for bladder cancers affected individuals improbable to tolerate MVAC because of renal purpose, era or even efficiency status: : Cisplatin 60 to 70 mg/m2 day 1 (or substitute carboplatin AUC 5) : Gemcitabine 1250 mg/m2 days to weeks 1+8 3) Concomitant chemo/radiotherapy. : Cisplatin 20mg/m2/daily by 5days together with 1 litre N Saline hydration. : Protect throughout full week 1 in addition to four associated with revolutionary the radiation concomitantly.
eMEDiCINE. Shah I; Gupta CL; Gupta 3rd there�s r; Bardwajs Section associated with Urology, Acharya Shri Chander College or university associated with Professional medical Sciences in addition to Infirmary, Sidhra, Jammu, Jammu-180006 (India) Transitional mobile carcinoma associated with bladder in small affected individuals JK-Practitioner. 2001 Jul-Sep; 8(3): 181-2. Warde P, Gospodarowicz MK: Completely new methods in the use of the radiation treatment in the management of infiltrative transitional-cell cancers from the bladder. Planet J Urol 1997; 15(2): 125-33.
Skin Cancer (Squamous Cell Carcinoma of the Skin)

Squamous Mobile Carcinoma from the Skin tone is a single kind of pores and skin cancer malignancy. Skin may be the most significant organ from the physique. This assists to be a safety filter involving all of us along with the natural environment, keeping drinking water with and an infection out there. Skin with constructed from a pair of key layers: The epidermis - comprising keratinised stratified squamous epithelium; along with the skin - any lustrous connective structure. Epidermal components of skin include the hair follicles and curly hair; perspiration, sebaceous and mammary glands; and claws. The actual features from the pores and skin include: Delivering any safety filter through the outside natural environment; Homeostasis - helping inside rules connected with body temperature and drinking water damage; Physical function - providing info on your outside natural environment; Excretion connected with physique essential fluids - perspiring; and Functionality connected with nutritional D in experience of sunlight. Moreover, tissue inside deep the main pores and skin help to make melanin to safeguard all of us from ultraviolet the radiation. From a cancer malignancy point of view, the key tissue inside pores and skin tend to be squamous tissue, basal tissue and melanocytes. It's the 2nd most frequent form of pores and skin cancer malignancy. This comes about having improving age having making love occurrence currently being more common with adult males. Geographically, your tumour can be found worldwide, however having stunning physical variance, having occurrence minimizing having improving distance through the equator. Squamous cellular carcinomas will be more popular with locations having large numbers of sunlight. The most important predisposing consider your development connected with squamous cellular carcinoma may be the experience of ultraviolent the radiation (UVB) sunlight. Serious experience of sunlight is connected with rapid growing older, blunting from the immunological responses from the pores and skin in order to environemnstal antigens along with the development connected with premalignant and malignant neoplasms. Even so, additionally, there are important genetic advantages towards development connected with squamous cellular carcinoma. Risk variables in relation to direct exposure and susceptability in order to sunlight include: reasonable pores and skin, Northern Western european ancestory, child years freckling and the quantity of beyond sunburns. Squamous cellular carcinoma may be the pores and skin cancer malignancy many carefully connected with cumulative solar direct exposure. Different predisposing variables include: Ionising the radiation, chemical substance cancerous carcinogens for example tobacco smoke and betel nut gnawing (particularly inside lips and about the lips), long-term immunosuppression (incidence connected with squamous cellular carcinoma much in excess of that will connected with BCC), unusual genetic ailments for example xeroderma pigmentosa, along with the People Papilloma Virus (HPV) which has been found in colaboration with a few cutaneous SCC. Squamous cellular carcinoma, in particular, is situated in affected individuals subsequent organ transplantation. SCC may also come up with areas of skin damage (known since Marjolin's ulcer) because of can burn, long-term ulcers or perhaps nose tracts. Such a tumour distributes by lymphatic infiltration having distribute in order to regional lymph nodes. Systemic distribute comes about in the future throughout the condition. Common deliberate or not might indicate simply no abnormality having the majority squamous cellular carcinomas. Squamous cellular carcinoma from the pores and skin is of a great diagnosis, having below 5% connected with skin lesions featuring proof regional lymph node metastases from examination. Having proper treatment your 5 yr illness no cost emergency pace is in very least 95%. Much like many malignancies, the sooner your point from examination, the better your diagnosis. Treating decision for squamous cellular carcinoma is surgical excision to a perimeter connected with at least 0. 5cm both equally in depth and laterally. Basic excision provides heal prices of approximately 90% though Moh's surgery is connected with heal prices connected with all around 97%. Adjuvant radiotherapy can be employed when the margins tend to be jeopardized by nearby important set ups. Radiotherapy is additionally connected with great heal prices however is reserved for affected individuals incapable of endure surgical excision. Interferon and photodynamic remedy tend to be more modern experimental treatment techniques currently being investigated. Advancement with signs can be an important description. Specific monitoring could possibly be by specialized medical follow-up in order to find repeat or perhaps the looks connected with fresh major skin lesions. This certainly will include visual examination and palpation for any further repeat or perhaps lymphatic distribute, along with asking yourself your affected individuals in relation to any kind of improved sensation in the region from the lesion. The actual signs that may call for consideration tend to be somatic pain from bony infiltration and neurogenic pain when neurological structure is compressed. Visceral pain from metastatic illness could also take place..
Osteosarcoma (Osteogenic sarcoma)
Osteosarcoma is a form of navicular bone cancers. Your your bones on the physique undoubtedly are a specialist type of connective tissues of which style the majority of the human being skeletal system. These are composed of calcium mineral, phosphate and magnesium inside a structure associated with sort I collagen. How big this skeletal system does not often boost over and above puberty (when combination on the skeletal development discs occur) however navicular bone can be a hugely metabolically effective tissues considering frequent resorption, development and remodelling. Your A few significant features associated with navicular bone is so visible since: Mechanical- assist associated with tissue, attachment associated with muscle tissues and permitting activity on the physique; Metabolic- this navicular bone types this significant storage space reservoir intended for calcium mineral and phosphate chemistry; and Protective- your bones give you the protecting ouert shell intended for critical body organs and as well to the navicular bone marrow. It's is uncommon, information technology at under 0. 2% associated with fresh malignancies on a yearly basis. Nevertheless, it does not take most common principal malignant navicular bone tumour. Almost all bony malignancies tend to be metastatic. A lot more than 75% come about within people youthful when compared with 19 years (with peaks from 10-14 for ladies and 15-18 intended for boys) however a second more compact top additionally takes place in the older having making love incidence as a doubly popular within males. Geographically, this tumour is located worldwide. Anatomical components engage in a fundamental part in the improvement associated with osteosarcoma. Heritable mutations in the p53 germline tend to be for this autosomal recessive Li Fraumeni affliction associated with familial cancer and people having mutations in the Rb gene (associated with the improvement associated with retinoblastoma) will also be with a risky associated with establishing osteosarcoma. Osteosarcoma additionally appears with an increase of frequency within people having osteogenesis imperfecta. Other predisposing components include: Elements of fast navicular bone development (as recommended from the location associated with tumours from web-sites associated with maximum navicular bone development and within elements of Paget's disease); and light (especially post-radiotherapy for any solid wood tumour within childhood). This sort of tumour advances by vascular intrusion and haematogenous dissemination. Lung and faraway navicular bone metastases tend to be the most prevalent web-sites intended for multiply. Common investigations may perhaps show anaemia or perhaps minimal platelet count when navicular bone marrow is concerned. Abnormal alkaline phosphatase quantities may be recognized. Before improvement associated with chemotherapeutic strategies this diagnosis by osteosarcoma seemed to be globally poor, that has a 5 12 months survival fee associated with less than 20%. Nevertheless, some sort of localized osteosarcoma is actually associated with a 5 12 months survival fee of around 60%. Remedy intended for osteosarcoma centers all around precise excision and chemotherapy. Surgical procedures will take the proper execution associated with both amputation or perhaps, within much less advanced instances, limb repair methods where by nearby resection is conducted. Often chemotherapy is used preoperatively in the expect that the non-resectable tumour demanding amputation can be shrunk as well as a nearby resection conducted. Your benefits associated with combination chemotherapy strategies and associated with limb sparing surgeries possess considerably decreased this death rate and morbidity associated with osteosarcoma. Enhancement within signs and symptoms is surely an important dimension. Specific keeping track of may be by serial CT and radioisotope navicular bone scanning to the discovery associated with frequent ailment. Your chest should likewise possibly be checked having serial x-rays as it might possibly be doable for you to resect actually numerous secondaries by a great osteogenic sarcoma. Your signs and symptoms that could require consideration tend to be somatic agony by navicular bone metastases, visceral agony by hardworking liver or perhaps lung metastases and neurogenic agony when neurological tissues is pressurized. Coughing and breathlessness by lung participation may require particular treatment. Osteosarcoma is radioresistant, therefore, light therapies doesn't have a part within regime supervision. (Source: Jesse Dalley: E Vincent's Hospital).


Primitive neuroectodermal tumour of the brain (PNET)
") Primitive neuroectodermal tumours (PNET) form a rare group of tumors defined by their appearance - they consist of small round cells in the nervous system. They are thought to develop from primitive or undifferentiated (having the potential become many different types of cell) nerve cells in the brain. Incidence is uncertain because PNETs are rare. They are usually described as a 'tumour of childhood'. In one study the average age of diagnosis was between 3 and 8 years. Although cancer is rare in children, brain tumors are the most common type of childhood cancer other than leukemia and lymphoma. Researchers have not been able to find an identifiable cause or risk factors for PNET. Most cases of PNET appear to happen spontaneously as the result of a mutation in the DNA.There doesn't appear to be a genetic predisposition, meaning the disease does not seem to run in families. Certain conditions have an increased association with PNETs. These include: Li-Fraumeni syndrome, Turcot syndrome and Gorlin syndrome. Tumours invade and destroy normal tissue, causing damage to sensory and cognitive functions of the brain. Increased intracranial pressure may result from the enlarging tumour mass, cerebral oedema (accumulation of fluid in the brain caused by swelling) and the obstruction of cerebrospinal fluid drainage (fluid that circulates throughout the brain and spinal cord). The only way to confirm a PNET is by taking a sample of the affected tissue and examining it under a microscope. An MRI scan or CT scan is usually performed to identify the location of the cancer and how far it has spread. The prognosis (chance of recovery) depends on: time of diagnosis (the earlier the better). age of the patient. Size and spread of the tumour before surgery. Cancer cells remaining after surgery.There are usually many health professionals involved in the care of someone with a brain tumour. These include a neurologist, neurosurgeon, radiation oncologist and medical oncologist. The main types of treatment include surgery, radiation therapy and chemotherapy. Surgery is usually used to make a diagnosis and improve symptoms. Radiation therapy is usually given in combination with another form of therapy, such as surgery, and has been shown to improve outcomes. Chemotherapy is usually administered in combination with radiotherapy
Primitive neuroectodermal tumours (PNET) form a rare group of tumors defined by their appearance - they consist of small round cells in the nervous system. They are thought to develop from primitive or undifferentiated (having the potential become many different types of cell) nerve cells in the brain. Incidence is uncertain because PNETs are rare. They are usually described as a 'tumour of childhood'. In one study the average age of diagnosis was between 3 and 8 years. Although cancer is rare in children, brain tumors are the most common type of childhood cancer other than leukemia and lymphoma. Researchers have not been able to find an identifiable cause or risk factors for PNET. Most cases of PNET appear to happen spontaneously as the result of a mutation in the DNA.There doesn't appear to be a genetic predisposition, meaning the disease does not seem to run in families. Certain conditions have an increased association with PNETs. These include: Li-Fraumeni syndrome, Turcot syndrome and Gorlin syndrome. Tumours invade and destroy normal tissue, causing damage to sensory and cognitive functions of the brain. Increased intracranial pressure may result from the enlarging tumour mass, cerebral oedema (accumulation of fluid in the brain caused by swelling) and the obstruction of cerebrospinal fluid drainage (fluid that circulates throughout the brain and spinal cord). The only way to confirm a PNET is by taking a sample of the affected tissue and examining it under a microscope. An MRI scan or CT scan is usually performed to identify the location of the cancer and how far it has spread. The prognosis (chance of recovery) depends on: time of diagnosis (the earlier the better). age of the patient. Size and spread of the tumour before surgery. Cancer cells remaining after surgery.There are usually many health professionals involved in the care of someone with a brain tumour. These include a neurologist, neurosurgeon, radiation oncologist and medical oncologist. The main types of treatment include surgery, radiation therapy and chemotherapy. Surgery is usually used to make a diagnosis and improve symptoms. Radiation therapy is usually given in combination with another form of therapy, such as surgery, and has been shown to improve outcomes. Chemotherapy is usually administered in combination with radiotherapy. [1] Ghosh S. Primitive neuroectodermal tumours of the central nervous system. eMedicine 2001. [available online: http://www.emedicine.com/neuro/topic326.htm][2] National Cancer Institute: Childhood Supratentorial Primitive Neuroectodermal Tumors and Pineoblastoma treatment. [available online: http://www.nci.nih.gov/cancertopics/pdq/treatment/childSPNET/Patient/page2][3] Osanai M, Yamaguchi J, et al. Unique cellular features of peripheral primitive neuroectodermal tumour. Med Electron Microsc 2004; 37: 193-197.[4] The Merck Manual of Diagnosis and Therapy: Chapter 177. CNS Neoplasms. [available online: http://www.merck.com/]
Tumour Lysis Syndrome
Tumour lysis syndrome is the name given to a collection of metabolic abnormalities that occur following the initiation of cytotoxic chemotherapy. This potentially lethal syndrome is most likely to occur in patients with bulky, rapidly proliferating tumours that are responsive to therapy. The most common malignancies it is associated with are leukaemias, high-grade non-hodgkin's lymphoma and Burkitt lymphoma, although it has been associated with other haematological and solid malignancies. Clinically, tumour lysis syndrome occurs in about 6% of patients being treated for non-hodgkin's lymphoma, but laboratory parameters consistent with it are seen in up to 42% of patients. The cells that make up cancer are often numerous and rapidly proliferating. There are therefore large numbers of them to be killed, and chemotherapy aims to do this quickly. As such large numbers are killed at the same time, their contents are rapidly and simultaneously released into the bloodstream. As a result, tumour lysis syndrome may occur and usually does so within 1-5 days of chemotherapy. Very occasionally, tumour lysis syndrome occurs spontaneously, with no exposure to chemotherapy agents. Tumour lysis syndrome causes a triad of hyperkalaemia, hyperphosphataemia and hyperuricaemia and leads to acute renal failure. Recognition of at-risk patients and the prevention of tumour lysis syndrome are the most important aspects of management. Pre-treatment hyperuricaemia and high lactate dehydrogenase levels represent a high tumour load, and therefore an increased risk for developing tumour lysis syndrome. Patients with pre-existing renal impairment are also at higher risk. All patients at high risk of tumour lysis syndrome should have electrolytes and kidney function monitored prior to chemotherapy and for 48-72 hours following therapy. This way any abnormalities will be detected early and renal failure may be prevented. Morbidity and mortality are related to acute renal failure, cardiac arrhythmias (due to hyperkalaemia) and metabolic acidosis. Tumour lysis syndrome is often predictable, and close monitoring of at-risk patients usually allows for effective treatment or even prevention. Allopurinol, urinary alkalinisation and aggressive hydration aim to reduce plasma uric acid levels and prevent renal failure. Rasburicase can be used if allopurinol is ineffective. Prophylaxis may also include limiting of potassium and phosphate intake. Due to the unpredictability of chemotherapy, tumour lysis syndrome may still occur despite aggressive prophylaxis. If signs develop, monitoring should continue at least twice daily. The appearance of renal failure in a patient with cancer does not immediately indicate tumour lysis syndrome. As mentioned earlier, there are many other causes of renal impairment in cancer patients. However, the appearance of all the aforementioned electrolyte disturbances plus renal failure, relatively soon after chemotherapy drugs have been administered, strongly suggests tumour lysis syndrome. If prevention has been unsuccessful or was not instituted, tumour lysis syndrome requires aggressive treatment. Therapy is aimed at maximising excretion of released intracellular products and minimising production of uric acid. Patients may require treatment in an oncology unit or ICU due to the need for continuous monitoring and specialist treatment. Laboratory results must be given priority and reviewed quickly to allow for rapid detection and correction of electrolyte imbalances. Regular cardiac monitoring using ECG should also be carried out, in order to detect any rhythm abnormalities should they occur. A coagulation profile should also be performed as part of early monitoring. Each electrolyte imbalance should be corrected individually, and the most important to address is the hyperuricaemia. Allopurinol is used, and can be given intravenously if the patient cannot tolerate it orally. If renal impairment is already obvious, dose reduction may be necessary. Rasburicase may be a useful alternative to allopurinol. It is faster, safe for use in children, and may reduce the need for dialysis. Urine alkalinisation should be performed to reduce uric acid precipitation. Sodium bicarbonate can be given intravenously to alkalinise urine. This prevents crystallisation of uric acid, and a pH of 7.0 is a reasonable aim. Care must be taken with this treatment, as calcium phosphate crystallises at an alkaline pH and an adjustment too far in that direction should be avoided. Regular urinary pH measurements should be used to guide alkalinisation therapy. Good urine flow helps prevent uric acid precipitation, but care should be taken not to fluid overload patients whose renal function is deteriorating. Hydration helps to correct electrolyte imbalances by diluting extracellular fluid. It also increases renal blood flow and encourages natural excretion of electrolytes. High-risk patients should be well hydrated prior to and during treatment, using intravenous fluids. This should be continued maintaining urine output of 3L/day unless the patient shows cardiac signs of volume overload. Proper fluid management is vital in preventing fluid overload and hypertensive complications. Diuretics should only be used in well hydrated patients showing signs of volume overload. Hyperkalaemia should be aggressively treated and monitored. Dietary potassium should be restricted, and potassium immediately removed from all intravenous fluids. Intravenous insulin + glucose helps redistribute potassium into the intracellular space. IV calcium gluconate can be used for cardio-protection if potassium levels exceed 6.5mmol/L. Potassium wasting diuretics should be used with caution as they may worsen renal precipitation. Oral potassium exchange resins should be given immediately, as this will outlast shorter-term treatments. Should all of these treatments fail to reduce potassium levels, dialysis is indicated. Oral phosphate binders (eg: aluminium hydroxide) should be used to control hyperphosphataemia. Hypocalcaemia usually resolves as phosphate levels are corrected. Hypocalcaemia should not be actively corrected (with calcitriol) unless Chvostek and Trousseau’s signs are positive. Dialysis may be indicated if the above measures fail to keep uric acid or phosphate levels below 10mg/dL. Haemodialysis is preferred, and may need to be repeated depending on results of ongoing monitoring. Dialysis helps prevent renal failure, and its preparation should be considered early in the course of the syndrome. The prognosis of tumour lysis syndrome is excellent with adequate treatment, with renal failure returning to normal when uric acid levels drop below 10mg/dL.
Treatment is first targeted at the specific metabolic disorder.
Acute renal failure prior to chemotherapy. Since the major cause of acute renal failure in this setting is uric acid build-up, therapy consists of rasburicase to wash out excessive uric acid crystals as well as a loop diuretic and fluids. Sodium bicarbonate should not be given at this time. If the patient does not respond, hemodialysis may be instituted, which is very efficient in removing uric acid, with plasma uric acid levels falling about 50% with each six hour treatment.
Acute renal failure after chemotherapy. The major cause of acute renal failure in this setting is hyperphosphatemia, and the main therapeutic means is hemodialysis. Forms of hemodialysis used include continuous arteriovenous hemodialysis (CAVHD), continuous venovenous hemofiltration (CVVH), or continuous venovenous hemodialysis (CVVHD).
Mantle cell lymphoma
Lymphoma is divided into 2 broad groups: Hodgkin's lymphoma and non-Hodgkin's lymphoma. Non-Hodgkin's lymphoma has many subtypes - and one of them is Mantle Cell Lymphoma. It is a B-cell lymphoma, which means it primarily affects the B lymphocytes. Lymphoma means cancer of the lymphatic system. The lymphatic system is important to our immune system where it helps to combat infection. The lymphatic system consists of several organs, e.g. lymph nodes, spleen, thymus and bone marrow, where all these are connected by tiny vessels. Lymphatic fluid is the medium that circulates in these tiny vessels. Like blood, it has cells in them. These cells can be divided into 2 types: T cells and B cells. The following figures are according to the Australian Institute of Health and Welfare: The incidence of non-Hodgkin's lymphoma is increasing over the years. In 2001, there were 3499 cases of non-Hodgkin's lymphoma reported in Australia. For non-Hodgkin's lymphoma, the male:female ratio is 1.22:1 In 2000, there were 2938 reported cases of B cell lymphoma (i.e. a subgroup of non-Hodgkin's lymphoma affecting primarily B lymphocytes) in Australia. B cell lymphoma is the commonest subgroup of non-Hodgkin's lymphoma.The male to female ratio for mantle cell lymphoma is 3 to 1.Most patients are in their sixties (around 63) when the disease is diagnosed. Of these, about 70% of the patients are in stage IV disease (see below regarding staging) Like most lymphomas, no causes has been found for mantle cell lymphoma. Yet based on statistics, several factors can be identified:Age: The disease mostly affects late middle age to elderly peopleSex: Male predominanceRace: Caucasians are affected more than Asians and Africans/African-Americans Clinically and historically, non-Hodgkin's lymphoma can be subdivided into 2 groups: indolent (low grade) and aggressive (high grade) lymphomas. Mantle cell lymphoma is under the indolent group - which means it has better prognosis but may not respond to treatment when compared to aggressive groups of lymphomas.As for the course of the disease, it is dependent on the clinical stage when the disease is diagnosed.The Ann-Arbor staging for non-Hodgkin's lymphoma (which is applicable for mantle cell lymphoma) can be summarised as below: Stage I - involvement of a single lymph node region or organ or site other than lymph nodes Stage II - 2 or more lymph node regions involved on the same side of diaphragm Stage III - 2 or more lymph node regions involved on both sides of diaphragm Stage IV - one or more organs (e.g. bone marrow) involvedEach stage is subclassified into A and B (e.g. IIA), where B means presence of B symptoms (see below) while A means abscence of the following symptoms: Unexplained a href="/symptoms.asp?sid=24">fever> 38 Centigrade Unexplained weight loss (defined as >10% of body weight in 6 months) Night sweats Mantle cell lymphoma is considered to be an indolent non-Hodgkin's lymphoma, which has better prognosis as compared to T cell lymphoma. Yet because 70% of the patients have stage IV disease at diagnosis (see incidence), mantle cell lymphoma has only moderate prognosis.The prognosis is dependent on the clinical stage when the disease is diagnosed. The later the stage, the worse the prognosis.The average survival for patients diagnosed with mantle cell lymphoma is 3 to 4 years.General investigations:The usual basic tests will be done, including those to look at the blood and other blood components. Other general tests will determine the function of the liver. Mantle cell lymphoma is a B-cell lymphoma, hence it is classified as an indolent lymphoma (see above). Although some patients may survive without treatment for many years, many patients present as aggressive lymphoma rather than an indolent one. While 'watchful monitoring' may the therapy of choice in some patients that do not have any symptoms, more aggressive treatment is usually adopted for patients with mantle cell lymphoma.The following treatment modalities can either be given alone or in combination: Chemotherapy: this is using chemical (drugs) to kill the cancer cells. One or more anti-cancer drugs may be used, but usually multiple drugs are used. Radiotherapy: this is using radiation to kill the cancerous cells. This is used when there is one or more lymph node regions affected in the same part of the body. Steroids: this is to reduce the side effects of anti-cancer drugs such as nausea and vomiting. Allogenic stem cell transplantation: this is first killing the cancer cells and normal lymphatic cells with chemotherapy and radiation, then infusing the body with non-cancerous new stem cells (cells that are precursor to the lymphatic system cells). However, this is limited to selected patients only due to the side effect profile of such treatment. Monoclonal antibody therapy: monoclonal antibodies are drugs that recognise, target and attach to particular proteins on the surface of cancer cells. This can then stimulate the body's own immune system to destroy the cell. Sometimes if the disease is aggressive, a monoclonal antibody may be added to chemotherapy. The current monoclonal antibody used is rituximab
[1] Cancer in Australia 2001 [online]. 2004. [Cited 2005 September 14th]. Available from: URL: http://www.aihw.gov.au/publications/can/ca01/ca01-c03.pdf[2] Clinical and pathologic features of mantle cell lymphoma [online]. 2005. [Cited 2005 September 14th]. Available from: URL: http://www.utdol.com/application/topic.asp?file=lymphoma/15026[3] How common is lymphoma [online]. 2003. [Cited 2005 September 14th]. Available from: URL: http://www.lymphoma.org.au/content/?id=25[4] Treatment of mantle cell lymphoma [online]. 2005. [Cited 2005 September 14th]. Available from: URL: http://www.utdol.com/application/topic.asp?file=lymphoma/20074
Tonsil Cancer (Lymphoma of the Tonsil)
Tonsil cancer may be of the Lymphoma type and usually arise from the lymphatic cells which are found in the wall of the tonsils.The pharynx is the continuation of the nose and mouth. It is a muscular tube that continues downwards through the neck and is responsible for the passage of both air (to the larynx, trachea and lungs) and food (to the oesophagus and then stomach). The pathways for food and air cross over in the pharynx. In addition, the auditory canal opens onto the upper part of the pharynx. The walls of the pharynx are composed of fascia and muscle layers all lined by a mucous membrane. The pharynx is divided into three different areas based on anatomical location: the nasopharynx (behind the nose); oropharynx (behind the mouth); and the laryngopharynx (behind the larynx).The tonsils are a ring of lymphoid tissue around the upper part of the pharynx. They consist of the lingual tonsil in the posterior part of the tongue, the palatine tonsils and the pharyngeal tonsils. Lymphoid tissue acts as a barrier against infection. Tonsil cancer is uncommon, but lymphoma of the head and neck is the second most common site of extranodal (not occuring within the lymph nodes) disease after the gastrointestinal tract. It occurs with highest incidence in adulthood with sex incidence being slightly male predominant.Geographically, the cancerous tumor is found worldwide, with variation depending on the underlying cause. For instance, Burkitt's lymphoma is more common in Africa. The cause of most cases of Non-Hodgkin's lymphoma is unknown although a number of predisposing factors have been identified. These are: some types of NHL (e.g. Burkitt's lymphoma) have been shown to contain particles of the Epstein-Barr Virus; HIV/AIDS predisposes to NHL, possibly as a result of the immune suppression but the virus itself may be implicated; immune suppression from anti-rejection drugs; exposure to certain chemicals; previous anti-cancer treatment; and certain genetic and chromosomal abnormalities. This type of cancerous tumor spreads by local extension, particularly into the soft palate and destruction of adjacent tissue. Lymphatic invasion with spread to the cervical lymph nodes is almost universal at the diagnosis of tonsil cancer. Up to 60% of patients presenting with non-Hodgkin's lymphoma of the head and neck will have systemic disease. General investigations into tonsil cancer may show anaemia or abnormal liver function tests. If haemolysis is present, the serum haptoglobin level may be lowered. Low grade lymphomas are usually slow growing and therefore compatible with a long life expectancy. They are not usually curable, but normally respond to treatment with long remission periods achievable. High grade lymphomas usually respond rapidly to treatment and a good proportion are curable. Prognosis of tonsil cancer can vary widely depending on the lymphoma type. For example, follicular small cleaved cell lymphoma has an average survival of 9 years. Low grade lymphomas usually have a first remission lasting approximately 3 years. The cancer treatment options available in non-Hodgkin's lymphoma are radiotherapy and chemotherapy. If the cancerous tumor is highly localised to the tonsils or head and neck region, then the tonsil cancer treatment of choice is radiotherapy and is very effective. More advanced tonsil cancer will require systemic cancer treatment with chemotherapy, but may also include radiotherapy as part of the cancer treatment regime.As a general rule, low-grade non-Hodgkin's lymphoma is usually treated with chlorambucil and prednisolone. This has the effect of putting people into cancer remission for a variable period of time. The low-grade non-Hodgkin's lymphomas usually relapse, but also usually respond to re-treatment of the cancer.High-grade lymphomas are potentially curable with intensive chemotherapy. Some examples are given below:Cancer treatment for non-Hodgkin's lymphoma had not really changed much in 25 years until very recently. Rituximab, a specific monoclonal antibody against a protein found on B lymphocytes has brought the first major advance in treatment since CHOP was first used in the 1970s.Currently only available on the PBS in Australia for low-grade non-Hodgkin's lymphoma, haematology and oncology specialists are eagerly awaiting the results of trials involving rituximab plus chemotherapy for high-grade lymphoma. It is expected that rituximab will increase the effectiveness of chemotherapy for tonsil cancer.As every cancer patient is different, your treating specialist will be able to advise you on which treatment of tonsil cancer is best for you.Improvement in symptoms of tonsil cancer is an important measurement. Specific monitoring may be by measurement of the size of the involved lymph nodes. This may often be done with a simple ruler of tape measure if the nodes are easily felt e.g. in the neck. If the lymph nodes are deep inside, e.g. in the chest or abdomen, then imaging such as CT scanning can show the response to cancer treatment.The symptoms that may require attention are fatigue from anaemia, and pain from organ or bone involvement. Radiotherapy is used for treating specific problems that require focal therapy, such as bone pain from bone involvement or treating obstruction of the Superior Vena Cava (the large vein that drains the face and upper body).
Mediastinal (thymic) large B cell lymphoma
Mediastinal large B cell lymphoma is a type of non-Hodgkin's lymphoma. Lymphoma is cancer of the lymphatic system and can be subdivided into Hodgkin's and non-Hodgkin's lymphoma.Lymphatic system is an important part of our immune system that helps fight infection. It is composed of various organs e.g. lymph nodes, thymus (in the mediastinum - behind the breastbone), spleen and bone marrow. These are connected by a network of tiny lymphatic vessels. Lymph is a colourless fluid that circulates in the lymphatic system. It contains lymphocytes, which are white blood cells that fight infection. There are 2 types of lymphocytes: B cells and T cells. Mediastinal large B cell lymphoma is a cancer of B cells.Mediastinum is between the breast bone and the back bone. It is the space in the chest that contains all the organs of the chest (heart, oesophagus, trachea, thymus and some large vessels) except the lungs and pleurae (the layer covering the lungs). Mediastinal large B cell lymphoma arises from the thymus (a lymphatic organ in the lymphatic system) in the mediastinum. Mediastinal large B cell lymphoma makes up about 2-6% of all lymphomas.The majority of patients are very young - around 30 years when they are diagnosed.It is slightly more common in females than in males - this is opposite of other types of non-Hodgkin's lymphoma. The cause is unknown. It does not run in families or occur because of genetic changes. There does not seem to be a relation to toxic agents.It is non-infectious and cannot be passed on to other people. This is a tumour that grows very quickly and causes symptoms in the chest as described below. It is usually localised (confined to an area) when patients come to the doctor.It requires prompt treatment. If the disease comes back, it has often spread to other organs such as the liver, kidneys or brain. Blood will be drawn and sent to the laboratory to look at certain features: The number and nature of blood cells Liver function Kidney function Level of other substances in the blood e.g. lactate dehydrogenase (LDH) and beta-2 microglobulin (indicates poorer disease outcome if the levels are high) Level of proteins (e.g. alpha-fetoprotein and beta-HCG) to differentiate mediastinal large B cell lymphoma from another disease called mediastinal germ cell tumour that happens in males. Alpha-fetoprotein and beta-HCG will be raised in mediastinal germ cell tumour. Of all patients, 40-80% are cured with treatment.If the disease comes back after treatment, it normally happens in the first year after diagnosis. A patient who is disease-free for 2 years after initial diagnosis is likely to be cured.Patients who do not show good response to initial treatment or whose disease comes back may require intensive chemotherapy with tranplantation of bone marrow cells. About 30% of this group will eventually stay free of the disease. The usual treatment is chemotherapy. The most commonly used combinations of drugs are the CHOP regimen and MACOP-B regimen. Treatment may last from 3-6 months.Most patient respond well to initial therapy. Response is assessed by performing scans.However, in some patients, the disease comes back in about one year. These patients may require intensive chemotherapy with transplantation of bone marrow cells.Steroids are usually given together with chemotherapy to help reduce feelings of sickness. Side effects from chemotherapy include nausea, vomiting, hair loss, infection and fever. Nausea and vomiting can be relieved by drugs.After the chemotherapy, radiotherapy is sometimes given to the mediastinal area.
Oral Cancer (Squamous Cell Carcinoma of the Floor of the Mouth)
Oral Cancer (Squamous Cell Carcinoma of the Floor of the Mouth) in oncology squamous cell cancers of the head and neck are often considered together because they share many similarities - in incidence, cancer type, predisposing factors, pathological features, treatment and prognosis. Up to 30% of patients with one primary head and neck tumour will have a second primary malignancy. The oral cavity or mouth consists of two parts: the vestibule, which is the space between the lips and cheeks and the teeth and gums; and the mouth proper which is internal to the teeth. The oral cavity refers to the entire contents of this area - including the cheeks, gums, teeth, tongue and palate. The functions of this region include ingestion, the first phases of digestion of food (mechanical destruction by the teeth through chewing), taste, respiration and the function of speech (with the movements of the oral cavity and its components shaping the sounds produced by the larynx into words). The floor of the mouth is the area between the mandible (jaw bone) and the attachment of the muscles of the tongue. It is lined by a thin mucous membrane and contains the sublingual salivary glands and the lingual frenulum (a loose attachment to the tongue).
Oral cancer is relatively common, with 3% of all malignancies arising within the oral cavity, and it occurs with increasing age. It is uncommon before the age of 40, and the highest incidence of oral cancer is in the 6th and 7th decades with sex incidence being a 2:1 male predominance. Geographically, the oral cacner tumour is found worldwide, but there is significant variation in incidence. Oral cancer occurs with highest incidence in African and Asian countries.
All oral cancers show a strong association with alcohol consumption and tobacco smoking, particularly of cigarettes - in fact, tobacco is thought to be implicated in well over 80% of cases of oral cancers. Chronic exposure of the epithelial surfaces of the head and neck to these irritants are thought to result in a "field cancerisation" sequence of hyperplasia, dysplasia and carcinoma. That is, the development of premalignant lesions that may then undergo malignant change to become an oral cancer. Smoking and alcohol act synergistically in the development of oral cancer - the risk when both of these factors is present is more than double the risk of exposure to one factor alone. There is a dose-response relationship between exposure to tobacco smoke and the development of oral cancer - the more you smoke the greater the risk of oral cancer. Smokers are up to 25 times more likely to develop head and neck cancer than their non-smoking counterparts. Passive smoking, tobacco chewing and cigar smoking are also risk factors for the development oral cancer. Up to the point of development of overt carcinoma, many of the changes associated with cigarette smoking will reverse if the patient quits smoking. Alcohol consumption as a risk factor for the development of oral cancer also shows a dose-response relationship - with heavy drinkers being at greater risk. In addition, drinkers of spirits may be at a greater risk than those who drink wine. Chronic viral infection is also associated with the development of oral cancer. Epstein-Barr Virus is strongly associated with the development of nasopharyngeal cancer, whilst Herpes Simplex Virus and Human Immunodeficieny Virus have been associated with the development of a number of different oral cancers. This is thought to be due to their interference with the function of tumour suppressor genes and oncogenes. HPV 16 and 18 are particularly associated with cancers of the oral cavity. Other risk factors or oral cancer include immune deficient states (such as post solid-organ transplant); occupational exposures to agents such as asbestos and perchloroethylene; radiation; dietary factors; a genetic predisposition to the development of oral cancer; and poor oral hygiene. Cancers of the oral cavity occur with highest incidence in countries where the betel nut is chewed. With cancers of the lips, sun exposure is an additional risk factor in development.
This type of tumour spreads by local extension and the destruction of adjacent tissue, with invasion of the tongue and mandible common. Lymphatic invasion with spread to the cervical lymph nodes is common at diagnosis. Haematogenous spread to distant sites such as the liver, bones and lungs may also have occurred at the time of diagnosis.
Oral cacner general investigations may show anaemia or abnormal liver function tests if the disease is very advanced, or due to the aetiology of the oral cacner. General investigations in the early stage of cancer ot the oral cavity tend to be normal.
Early oral cancer diagnosis is the key prognostic factor in cancer - of the floor of the mouth - influencing both tumour size and the likelihood of metastatic deposits. The 5 year disease free rate is approximately 70% in early oral cancer, falling to less than 30% in more advanced cases. Furthermore, aetiological factors associated with tongue cancer (primarily smoking and alcohol) render survival worse for patients than for other malignancies. The "field cancerisation" concept means that they are at increased risk of developing second primary oral tumours in the head and neck region, as well as being at significant risk from cardiovascular and liver disease associated with their lifestyle.
Treatment of oral cancer revolves around a combination of surgery and radiotherapy. Lesions should be treated surgically where possible because of the risks of bone necrosis with radiotherapy. Excision can be very difficult due to the proximity of the mandible. Where surgery is not possible, radiotherapy can be used - either with curative intent or for palliation. Post-operative radiotherapy may also be used. Bleomycin and cisplatin have both been used in the treatment of oral cancer. Improvement in oral cancer symptoms is an important measurement. Specific monitoring may be by thorough serial inspection of the head and neck region - looking for oral cancer recurrence as well as second primary oral tumours. Ideally this would include pan- /triple-endoscopy. There are no specific screening recommendations at the moment but several clinical trials are currently being undertaken into the benefit of different screening techniques. The oral cancer symptoms that may require attention are somatic pain from bone metastases, visceral pain from liver or lung metastases and neurogenic pain if nerve tissue is compressed. Coughing and breathlessness from lung involvement may require specific treatment.
Labels:
Meningioma,
Spinal
Meningioma of the Spinal Cord
 Meningioma of the Spinal Cord is a type of spinal cord cancer.The spinal cord forms part of the central nervous system. It is a cylindrical continuation of the brainstem, commencing from the medulla (at the level of the foramen magnum at the base of the skull) and extending to the conus medullaris at the level of the L2 vertebra. It is located within the vertebral canal - the bony tube formed by the vertebral foramina. Below the level of L2 the remaining contents of the spinal canal are known as the cauda equina - the bundle of nerve rootlets in the subarachnoid space. Within the vertebral canal run the spinal cord, the spinal meninges, the cerebrospinal fluid, associated vessels and loose connective and fatty tissue. The spinal meninges - the dura, arachnoid and pia mater - are membranes surrounding and supporting the spinal cord.Arising from the spinal cord are 31 pairs of spinal nerves that are the neural connections between the peripheries and the central nervous system. They attach to the spinal cord through ventral and dorsal roots and have both afferent and efferent properties. That is, the spinal cord acts as the main pathway for communication between the brain and the rest of the body.Tumours of the spinal cord can be either primary or metastatic. The vast majority of spinal cord tumours are metastatic deposits from other primary sites. Tumours of the spinal cord can be divided into three groups, based on the anatomical location of the tumour mass. Firstly, they are divided by their relationship to the spinal meninges, with tumours being classified as intradural or extradural. Furthermore, intradural tumours can be subdivided into those arising within the substance of the spinal cord itself - intramedullary tumours - or those arising in the subarachnoid space (extramedullary).Extradural tumours most commonly represent metastases and usually arise within the vertebral bodies. These tumours most commonly cause spinal compression through extrinsic mass effect but can on occasion do so through intradural invasion. Symptoms from these tumours tend to be the slowly progressing features of spinal cord compression with initial predominantly motor loss followed by progressive sphincter dysfunction and ascending sensory loss. Extradural tumours represent the vast majority of spinal cord tumours.Intradural extramedullary tumours tend to be nerve sheath tumours (neurofibromas) or meningiomas. They commonly present with nerve root involvement consisting of pain and progressive dysfunction due to spinal cord compression from the expanding tumour mass.Intramedullary tumours usually represent gliomas - ependymomas or astrocytomas - but metastatic deposits within the spinal cord itself are increasingly recognised. These tumours result in a diffuse swelling of the spinal cord, often over several segments, characterised by loss of local function, pain and eventual loss of spinal cord function below the level of the lesion. A cyst may form in the spinal medulla, giving rise to a clinical picture of syringomyelia (predominant loss of spinothalamic function - pain and temperature sensation - and blunted reflexes at the level of the lesion). Sacral sparing is a very late feature of intramedullary tumours but is pathognomonic. It is rare with less than 1.5 per 100,000 primary spinal cord tumours and of these only approximately 1/4 are meningiomas. More than 90% of meningiomas arise within the cranial fossa and occurs with highest incidence in patients aged 40 to 70 years with sex incidence being 3:1 female to males, except when the tumour occurs in children where the sex incidence is approximately equal. Meningiomas tend to increase in size during pregnancy.Geographically, the tumour is found worldwide. The only proven risk factor in the development of meningioma is exposure to ionising radiation - with tumours commonly developing following a 10 to 20 year lag time from exposure. Patients with neurofibromatosis type 2 (genetic defect on chromosome 22) are at increased risk of developing meningioma. This type of tumour spreads by local invasion and erosion of surrounding bony structures through pressure effects. Meningiomas are very rarely malignant but occasionally tumours may show a tendency to recur. General investigations may show no abnormality on routine blood and other investigations. Benign meningiomas are associated with a very good survival prognosis with approximately 100% 5 year survival. Morbidity relates to the location of the tumour and the degree of neurological dysfunction at diagnosis. Malignant meningiomas have a poor prognosis with median survival of between one and three years even with treatment. Initial treatment of patients with suspected spinal cord compression is with corticosteroids.Surgical resection is the mainstay of treatment in meningiomas of the spinal cord and the degree to which a tumour can be resected has great bearing on prognosis. Unfortunately, the recovery of previously lost neurological function post-operatively is unlikely.Where complete resection is not possible, post-operative radiotherapy is limited to the area of the tumour and the margin of potential spread is advocated in preference to more radical surgical approaches which are associated with significant increases in post-operative morbidity without any clear survival benefit. Tumour recurrence is usually treated with further surgery.Improvement in symptoms is an important measurement. Specific monitoring may be done by serial neurological examination and imaging of the spinal cord.The symptoms that may require attention are those resulting from the neurological deficits associated with the tumour, and the neurogenic pain from compressed nerve tissue. Patients with significant neurological deficits are best managed by a specialised neurological team, using a multidisciplinary approach including physiotherapy, occupational therapy, nursing and medical practitioners.
Meningioma of the Spinal Cord is a type of spinal cord cancer.The spinal cord forms part of the central nervous system. It is a cylindrical continuation of the brainstem, commencing from the medulla (at the level of the foramen magnum at the base of the skull) and extending to the conus medullaris at the level of the L2 vertebra. It is located within the vertebral canal - the bony tube formed by the vertebral foramina. Below the level of L2 the remaining contents of the spinal canal are known as the cauda equina - the bundle of nerve rootlets in the subarachnoid space. Within the vertebral canal run the spinal cord, the spinal meninges, the cerebrospinal fluid, associated vessels and loose connective and fatty tissue. The spinal meninges - the dura, arachnoid and pia mater - are membranes surrounding and supporting the spinal cord.Arising from the spinal cord are 31 pairs of spinal nerves that are the neural connections between the peripheries and the central nervous system. They attach to the spinal cord through ventral and dorsal roots and have both afferent and efferent properties. That is, the spinal cord acts as the main pathway for communication between the brain and the rest of the body.Tumours of the spinal cord can be either primary or metastatic. The vast majority of spinal cord tumours are metastatic deposits from other primary sites. Tumours of the spinal cord can be divided into three groups, based on the anatomical location of the tumour mass. Firstly, they are divided by their relationship to the spinal meninges, with tumours being classified as intradural or extradural. Furthermore, intradural tumours can be subdivided into those arising within the substance of the spinal cord itself - intramedullary tumours - or those arising in the subarachnoid space (extramedullary).Extradural tumours most commonly represent metastases and usually arise within the vertebral bodies. These tumours most commonly cause spinal compression through extrinsic mass effect but can on occasion do so through intradural invasion. Symptoms from these tumours tend to be the slowly progressing features of spinal cord compression with initial predominantly motor loss followed by progressive sphincter dysfunction and ascending sensory loss. Extradural tumours represent the vast majority of spinal cord tumours.Intradural extramedullary tumours tend to be nerve sheath tumours (neurofibromas) or meningiomas. They commonly present with nerve root involvement consisting of pain and progressive dysfunction due to spinal cord compression from the expanding tumour mass.Intramedullary tumours usually represent gliomas - ependymomas or astrocytomas - but metastatic deposits within the spinal cord itself are increasingly recognised. These tumours result in a diffuse swelling of the spinal cord, often over several segments, characterised by loss of local function, pain and eventual loss of spinal cord function below the level of the lesion. A cyst may form in the spinal medulla, giving rise to a clinical picture of syringomyelia (predominant loss of spinothalamic function - pain and temperature sensation - and blunted reflexes at the level of the lesion). Sacral sparing is a very late feature of intramedullary tumours but is pathognomonic. It is rare with less than 1.5 per 100,000 primary spinal cord tumours and of these only approximately 1/4 are meningiomas. More than 90% of meningiomas arise within the cranial fossa and occurs with highest incidence in patients aged 40 to 70 years with sex incidence being 3:1 female to males, except when the tumour occurs in children where the sex incidence is approximately equal. Meningiomas tend to increase in size during pregnancy.Geographically, the tumour is found worldwide. The only proven risk factor in the development of meningioma is exposure to ionising radiation - with tumours commonly developing following a 10 to 20 year lag time from exposure. Patients with neurofibromatosis type 2 (genetic defect on chromosome 22) are at increased risk of developing meningioma. This type of tumour spreads by local invasion and erosion of surrounding bony structures through pressure effects. Meningiomas are very rarely malignant but occasionally tumours may show a tendency to recur. General investigations may show no abnormality on routine blood and other investigations. Benign meningiomas are associated with a very good survival prognosis with approximately 100% 5 year survival. Morbidity relates to the location of the tumour and the degree of neurological dysfunction at diagnosis. Malignant meningiomas have a poor prognosis with median survival of between one and three years even with treatment. Initial treatment of patients with suspected spinal cord compression is with corticosteroids.Surgical resection is the mainstay of treatment in meningiomas of the spinal cord and the degree to which a tumour can be resected has great bearing on prognosis. Unfortunately, the recovery of previously lost neurological function post-operatively is unlikely.Where complete resection is not possible, post-operative radiotherapy is limited to the area of the tumour and the margin of potential spread is advocated in preference to more radical surgical approaches which are associated with significant increases in post-operative morbidity without any clear survival benefit. Tumour recurrence is usually treated with further surgery.Improvement in symptoms is an important measurement. Specific monitoring may be done by serial neurological examination and imaging of the spinal cord.The symptoms that may require attention are those resulting from the neurological deficits associated with the tumour, and the neurogenic pain from compressed nerve tissue. Patients with significant neurological deficits are best managed by a specialised neurological team, using a multidisciplinary approach including physiotherapy, occupational therapy, nursing and medical practitioners.
Non-Small Cell Lung Cancer (NSCLC)
Lung cancers are one of the most common cancers worldwide. Lung cancers are classified as either small cell lung cancer (SCLC) or non-small cell lung cancer (NSCLC).
Non-small cell lung cancers refers to a subset of cancer types that account for approximately 70% of lung cancers, including squamous cell carcinoma of the lung, large cell carcinoma of the lung, and adenocarcinoma of the lung.
Lung cancer is common. One in every 28 Australians will develop lung cancer during their lifetime. Lung cancer is also deadly: it is the most common cause of cancer death in Australia, accounting for around 23% of male and 15% of female cancer deaths. Lung cancer is more than twice as common in men as in women.
Geographically, the tumour is found worldwide, but it is especially common in countries with high tobacco consumption. As a group, non-small cell lung cancers make up about 70% of all lung cancers.
Cigarette smoking is the main predisposing factor. In recent years, it has been recognised that passive smoking (e.g. from a first degree relative in a house of smokers) can also put people at risk. Generally, the risk increases with the number of cigarettes smoked.
Exposure to asbestos increases the risk of developing this tumour. The combination of asbestos exposure plus cigarette smoking is particularly harmful. Other occupational exposures such as exposure to metals including arsenic, chromium and nickel can also increase risk.
Some studies have suggested that diet can play a role in lung cancer risk. Though it is not known how it works, diets high in fruits and vegetables seem to decrease risk.
Radiation exposure damages the DNA material within the cells and can also cause lung cancer. Radon (a radioactive gas) exposure from our normal surrounding environment, if higher than normal, can predispose to lung cancer. This evidence is mainly based upon population studies which show that people living in areas with a high radon content are prone to increased incidences of a variety of cancers.
Primary lung cancers are classified as either small cell tumours or non-small cell tumours. Non-small cell lung cancers include the subtypes squamous cell carcinoma of the lung, large cell carcinoma of the lung, and adenocarcinoma of the lung. These cancers are grouped together because they behave in a similar fashion, and, when diagnosed at an early stage, they may be cured by surgery.
As they grow, non-small cell lung cancers can spread to distant organs via the bloodstream or lymphatic vessels to the adrenal glands, liver, brain and bone.
Patients with lung cancer may notice:
Rarely, patients may present with difficulty swallowing or wheezing. Patients who have metastases (distant spread) at diagnosis may have symptoms related to this spread. For example, patients with cancer spread to the bone may experience bone pain or fractures.
Blood tests:
Imaging tests:
Chest x-ray: lung cancer may be seen on chest x-ray as a solitary pulmonary nodule or mass. As many as 80% of solitary pulmonary nodules (
") CT scanning: this is more accurate than chest x-ray, and may be particularly useful in identification of lymph node involvement. See the example image below.
CT scanning: this is more accurate than chest x-ray, and may be particularly useful in identification of lymph node involvement. See the example image below.") PET scanning can help to distinguish between benign and malignant solitary pulmonary nodules seen on chest x-ray. PET scanning may also be used in the assessment of nodal spread and metastatic disease.Imaging of other organs: if it is suspected that the cancer has spread to other organs, scans of the liver, brain or bone may be required.
PET scanning can help to distinguish between benign and malignant solitary pulmonary nodules seen on chest x-ray. PET scanning may also be used in the assessment of nodal spread and metastatic disease.Imaging of other organs: if it is suspected that the cancer has spread to other organs, scans of the liver, brain or bone may be required.While imaging tests are helpful in raising the suspicion of lung cancer, diagnosis requires that cancer cells are seen under a microscope. There are a number of ways of obtaining samples of suspected cancer cells:
Sputum cytology: cells from the sputum (spit) are examined for signs of malignancy (cancer)Bronchoscopy with washings, brushings and biopsy: a bronchoscopy is a camera tube placed through the throat into the airways of the lungs. Samples of the cells from the airways can be taken with washing, brushing, or biopsy.Fine needle aspiration biopsy through the skin may be used to investigate suspected lung tumours located near the edges of the lungs.
The prognosis (probable outcome) depends on the stage of the tumour. Cancer staging is a tool which allows prediction of patient outcomes, and helps decide on the best treatment options. It takes into account various features of a tumour in an individual patient, which can then be compared to other patients with similar tumour features.
Staging of non-small cell carcinoma of the lung is based on the TNM (Tumour, Node, Metastasis) system. 'Tumour' refers to tumour size, which is measured in centimetres. 'Node' refers to the presence of cancerous cells in regional lymph nodes. 'Metastasis' refers to the spread of cancer beyond regional lymph nodes to other organs of the body.
Tumour size (T): Tx: Primary tumour not able to be assessedT0: No evidence of primary tumour, ie. cancer cells seen on sputum sampling or bronchial washing onlyTis: Carcinoma in situT1: Tumour 3 cm or less, surrounded by pleura, without evidence of invasion more proximal than the lobar bronchus.T2: Tumour with any of the following features: >3cm in greatest dimensionInvolves main bronchus, 2cm or more distal to the carinaInvades visceral pleuraAssociated with atelectasis or obstructive pneumonitis, extending to the hilar region but not involving the entire lung.T3: Tumour of any size, directly invading the chest wall, diaphragm, mediastinal pleura or parietal pericardium; or tumour in the main bronchus; orin the main bronchus, less than 2cm distal to the carina, but without involvement of the carina; orwith associated atelectasis or obstructive pneumonitis of the entire lungT4: Tumour of any size, invading the mediastinum, heart, great vessels, trachea, oesophagus, vertebral body, carina; or with separate tumour nodules in one lobe, or with malignant pleural effusionRegional lymph nodes (N): NX: Regional lymph nodes not able to be assessedN0: No regional lymph node metastasisN1: Metastasis in ipsilateral peribronchial and/or ipsilateral hilar lymph nodes and intrapulmonary nodes, including involvement by direct extensionN2: Metastasis in ipsilateral mediastinal and/or subcarinal lymph nodesN3: Metastasis in contralateral mediastinal, contralateral hilar, ipsilateral or contralateral scalene, or supraclavicular lymph nodesDistant Metastasis (M) MX: Distant metastasis not able to be assessedM0: No distant metastasisM1: Distant metastasis, including separate tumour nodule(s) in a different lobe (ipsi- or contralateral).
Using this classification, non-small cell lung cancers are grouped into stages as follows:
Stage 0: TIS N0 M0Stage Ia: T1 N0 M0Stage Ib: T2 N0 M0Stage IIa: T1 N1 M0Stage IIb: T2 N1 M0, T3 N0 M0Stage IIIa: T1 N2 M0, T2 N2 M0, T3 N1 M0, T3 N2 M0Stage IIIb: any T N3 MO, T4 any N M0Stage IV: any T any N M1
Using this system, outcomes are best for patients with early stages of disease, with small tumours, no spread to lymph nodes, and no distant spread (metastasis) to other organs. Outcomes are also better for younger patients.
Overall, 5-year survival for all types of lung cancer in Australia is 11% for males and 14% for females. Survival for non-small cell lung cancer is better than for small cell lung cancer. Different subtypes of NSCLC are also associated with different survival rates. Survival is best for adenocarcinoma, followed by squamous cell carcinoma of the lung and large cell carcinoma.
Management of patients with lung cancer requires interaction from many medical specialties such as medical and radiation oncology, respiratory physicians, cardiothoracic surgeons, palliative care specialists, psychologists and physiotherapists. The main treatment modalities are surgery (such as lobectomy), chemotherapy and radiotherapy.
Surgical treatment
Surgery offers the best chance of cure, but is usually only possible with small tumours that have not yet spread (stage I or II). In some cases, lobectomy may be more appropriate than limited resection.If surgical treatment is to be given, the lymph nodes draining the tumour should be sampled and removed if the cancer has spread.
Radiotherapy
Patients with tumours which are not suitable for surgical resection can benefit from radiotherapy to the chest.Patients with early disease (Stage I or II cancer) who have had the tumour completely surgically removed do not usually need radiotherapy.
Chemotherapy
Chemotherapy can increase survival for patients with advanced cancer who are otherwise medically fit. Chemotherapy may also have improve quality of life for these patients.If chemotherapy is to be used, combination regimes (using more than one drug together) are better than single-drug regimes. Chemotherapy using platinum-based drugs produces the best results.
New classes of treatment agents, such as biological therapies, are finding a place alongside chemotherapy. Watch this site for breaking news regarding this treatment.
Palliative care
Lung symptoms commonly reported by patients with incurable lung cancer include shortness of breath from pleural effusion, coughing, or haemoptysis (coughing up blood). Pain may be from the lung tumour itself, or from spread (metastasis) to other organs, including bone. Treatment is available for all of these symptoms. In some cases, radiotherapy may be used to manage cancer pain. Spinal cord compression is a complication of cancer spread to the spine which requires urgent treatment.
Subscribe to:
Posts (Atom)





